Highlights
Tivdak (tisotumab vedotin) is a new drug indicated to treat adult patients with recurrent or metastatic cervical cancer that has progressed on or after chemotherapy.
Tivdak, developed by Seagen, called Seattle Genetics until October 2020, and Denmark’s Genmab, was approved by the U.S. Food and Drug Administration (FDA) in late September 2021. The regulator’s decision is conditional, meaning the drug has yet to be definitively confirmed for therapeutic efficacy.
For U.S. patients, the list price (without discounts and rebates) for a single 40-mg dose vial of Tivdak is set at $5,885. Because the total dose depends on body weight, the final cost of treatment varies; it could be about $34,000 for a one-month course of Tivdak.

Cervical Cancer Features
Although vaccination prevents cervical cancer in some cases, it is still the fourth most common and fourth most deadly cancer in women worldwide. [1] And the main contribution to deaths comes from recurrent or metastatic cervical cancer. [2]
Double platinum-containing chemotherapy has been the standard of first-line treatment. [3][4][5] The addition of Avastin (bevacizumab), endothelial growth factor (VEGF) inhibitor, prolonged overall survival, leading to a review of the standard of first-line therapy. [6] [7] However, intolerance and possible resistance associated with the regimens used limits their use and often leads to disease progression. [8]
Currently, there is no standard of second-line therapy for patients facing recurrent or metastatic cervical cancer. Thus, the widely used monotherapy with cytotoxic drugs is characterized by a poor benefit to risk ratio and low objective response rate (ORR < 15%). [9] [10] [11] [12] [13] [14] [15] In addition, there are very little data on the use of single-component chemotherapy after disease progression, having undergone first-line therapy with bevacizumab.
In June 2018, Keytruda (pembrolizumab) was approved for the treatment of recurrent or metastatic cervical cancer that progresses on or after chemotherapy and is characterized by the presence of PD-L1 tumor expression (CPS ≥1). A modest proportion of patients responded (ORR 14.3%) to the administration of this PD-1 blocker by Merck & Co., although the responses were long-lasting. [10] [16] Remarkably, the corresponding clinical trial KEYNOTE-158 (NCT02628067) was far from fully representative of the actual population of second-line patients, as less than half (42%) of subjects received bevacizumab and nearly all (94%) had disease characterized by squamous cell histology.
In October 2021, Keytruda received regulatory approval for the first-line treatment of persistent, recurrent, or metastatic cervical cancer with PD-L1 tumor expression (CPS ≥1). Pembrolizumab should be used in combination with chemotherapy drugs and bevacizumab (or without it). The addition of an immunotherapy agent to standard therapy, validated in the KEYNOTE-826 (NCT03635567) clinical trial, improved clinical outcomes including ORR, overall survival (OS), and progression-free survival (PFS). [17]
Given the lack of efficacy of existing second-line treatment options for recurrent or metastatic cervical cancer and the lack of a standard therapy for this indication, the physician and patient communities need new pharmacological treatment options that address alternative targets.
Tivdak: Mechanism of Action of Tisotumab Vedotin
Tisotumab vedotin is a antibody-drug conjugate (ADC) targeting tissue factor (TF) and carrying the cytotoxic monomethyl auristatin E (MMAE), an auristatin derivative and a strong microtubule disruptor.
Tissue factor, being a transmembrane protein and initiator of the coagulation cascade, is overexpressed by many tumor cells and epithelial cells of the tumor microenvironment. TF expression correlates with metastasis, angiogenesis, tumor cell growth, and tumor-associated thrombosis.
The antibody motif of tisotumab vedotin prevents TF from binding to coagulation factor VIIa (FVIIa) and prevents the activation of coagulation factor X (FX) into FXa. As a result, thrombin formation and the appearance of cancer-associated venous thromboembolism are inhibited, and angiogenesis and proliferation of tumor cells are suppressed.
After targeted delivery and internalization of the drug, the cytotoxic load MMAE is released as a result of proteolytic cleavage of the covalent linker. MMAE then binds to tubulin and inhibits its polymerization, resulting in G2/M phase arrest and apoptosis of malignant cells.
In vitro tisotumab vedotin also mediates antibody-dependent cell phagocytosis (ADCP) and antibody-dependent cellular cytotoxicity (ADCC).
Tivdak: Efficacy and Safety of Tisotumab Vedotin in Cervical Cancer Treatment
The innovaTV 204 (NCT03438396) phase 2 (non-randomized, open-label, multicenter, international) clinical trial enrolling adult patients (n=101) studied tisotumab vedotin monotherapy for cervical cancer characterized by extra-pelvic metastasis or recurrence, which progressed on or after standard platinum-containing chemotherapy with or without bevacizumab.
Subjects could receive no more than two lines of systemic therapy for recurrent or metastatic disease.
Patients were excluded if they had active ocular surface disease, any prior episode of cicatricial conjunctivitis or Stevens–Johnson syndrome (SJS), peripheral neuropathy grade ≥ 2, or known coagulation disorders with increased bleeding risk.
Among key patient characteristics: median age 50 years (31–78); 68% had squamous cell carcinoma, 27% had adenocarcinoma, and 5% had adenosquamous carcinoma; 70% had received one line of systemic therapy, 30% two; 69% had previously received bevacizumab.
Tivdak at an intravenous dose of 2 mg/kg every 3 weeks was administered until disease progression or unacceptable toxicity.
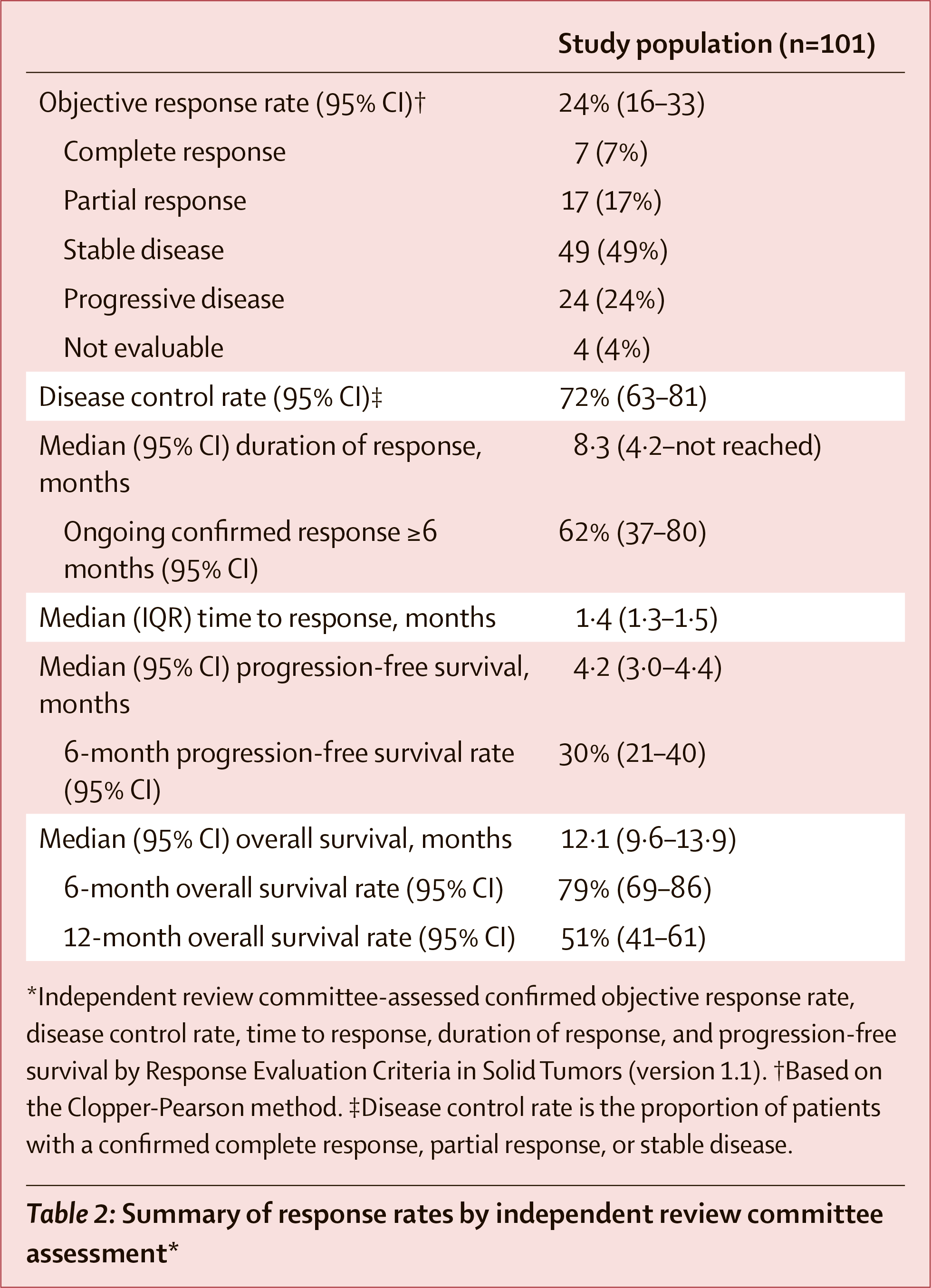
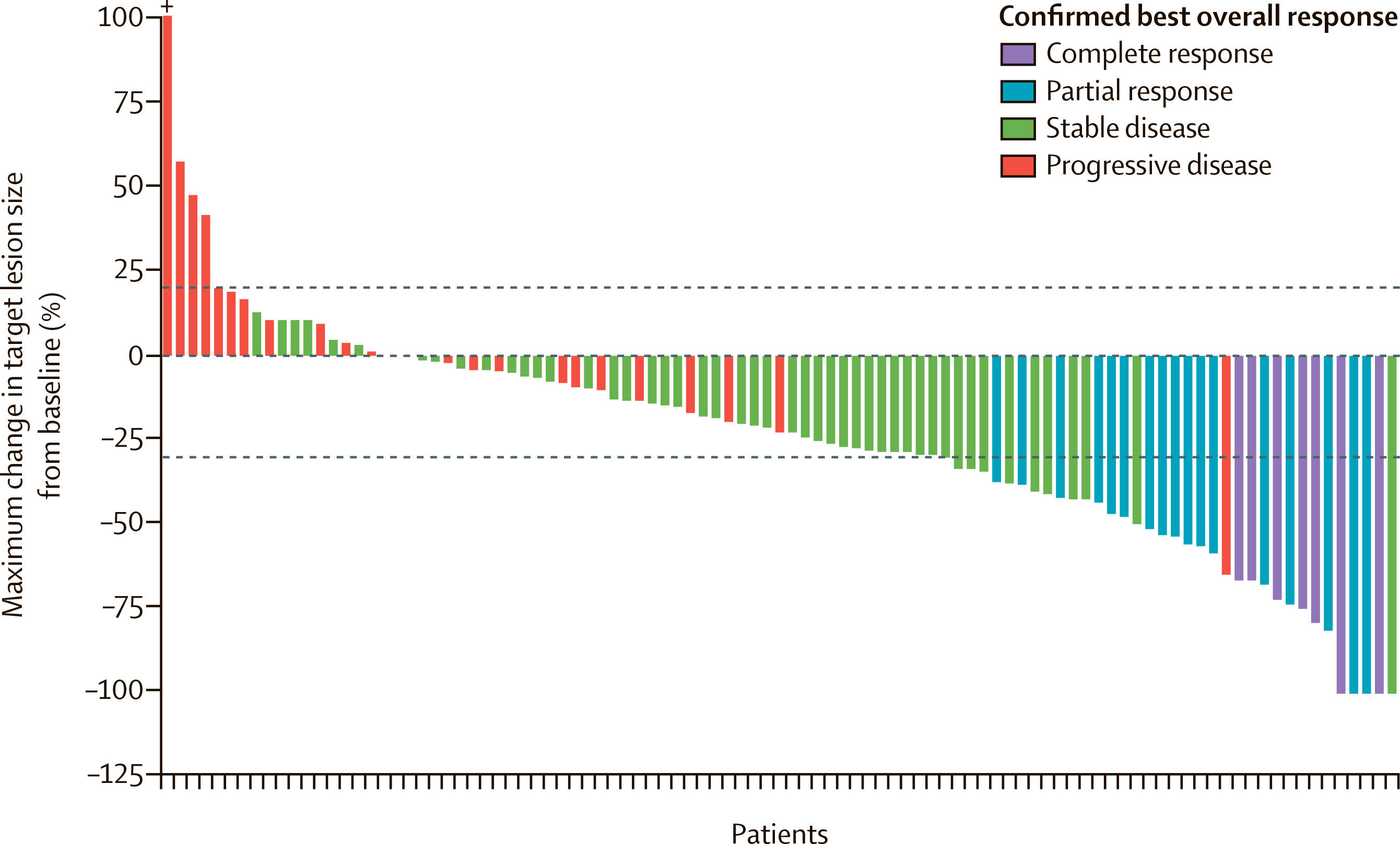
After a median of 10.0 months (interquartile range [IQR] 6.1–13.0]) of follow-up, the objective response rate (ORR) was 24% (95% CI: 16–33), including 7% complete responses (CR) and 17% partial responses (PR). The disease control rate (DCR), as the sum of CR, PR, and disease stabilization (SD) rates, came out to 72% (95% CI: 63–81).
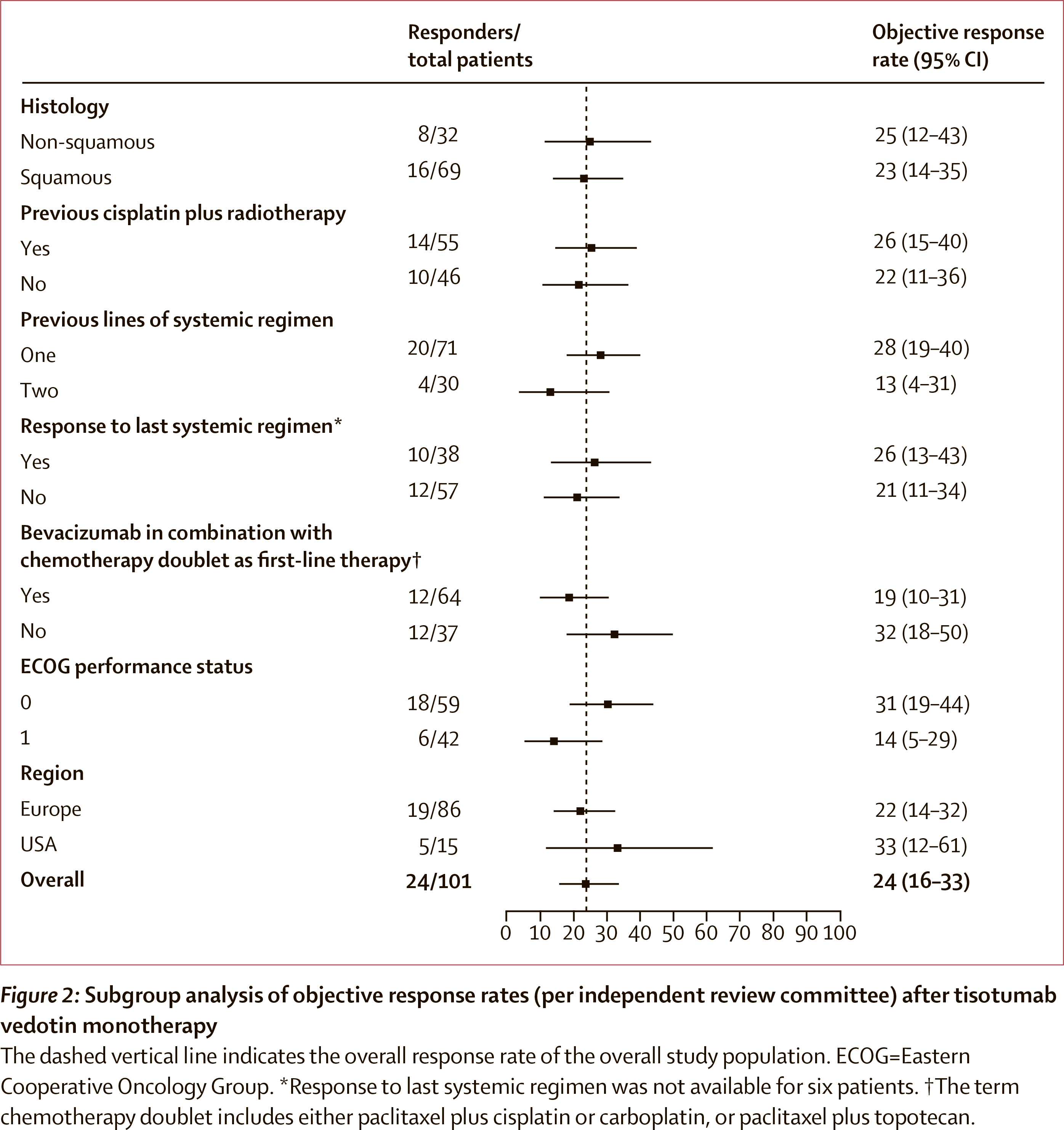
Response to treatment was documented regardless of tumor histology (squamous 23%, non-squamous 25%), number of lines of prior therapy (one 28%, two 13%), response to prior systemic treatment (with response 26%, without response 21%), prior bevacizumab administration (used 19%, not used 32%).
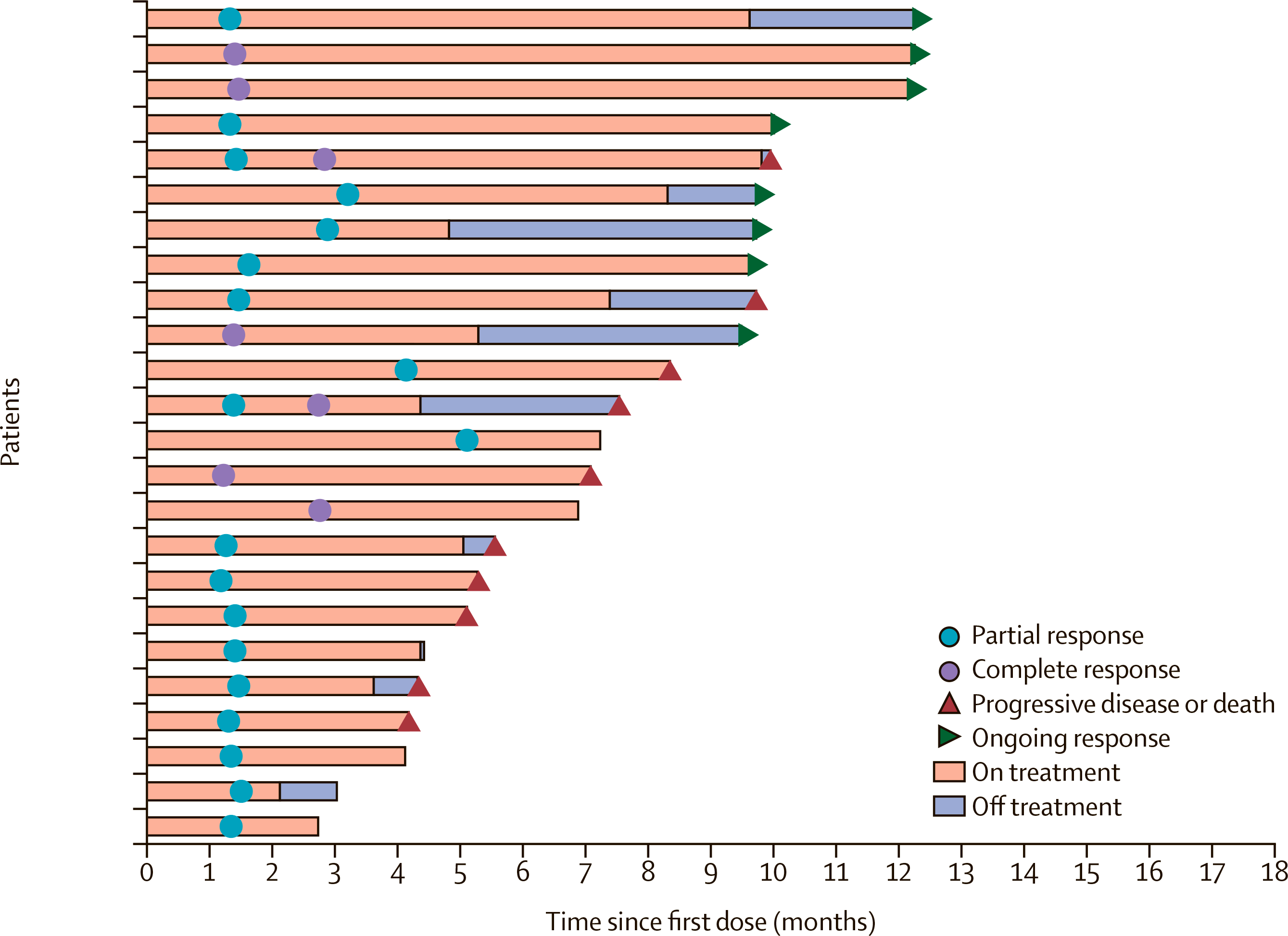
The median duration of response (DoR) was 8.3 months (95% CI: 4.2–NR), with a response of 6 months or longer in 62% (95% CI: 37–80) of respondents.
The median time to response (TTR) was 1.4 months (IQR 1.3–1.5).
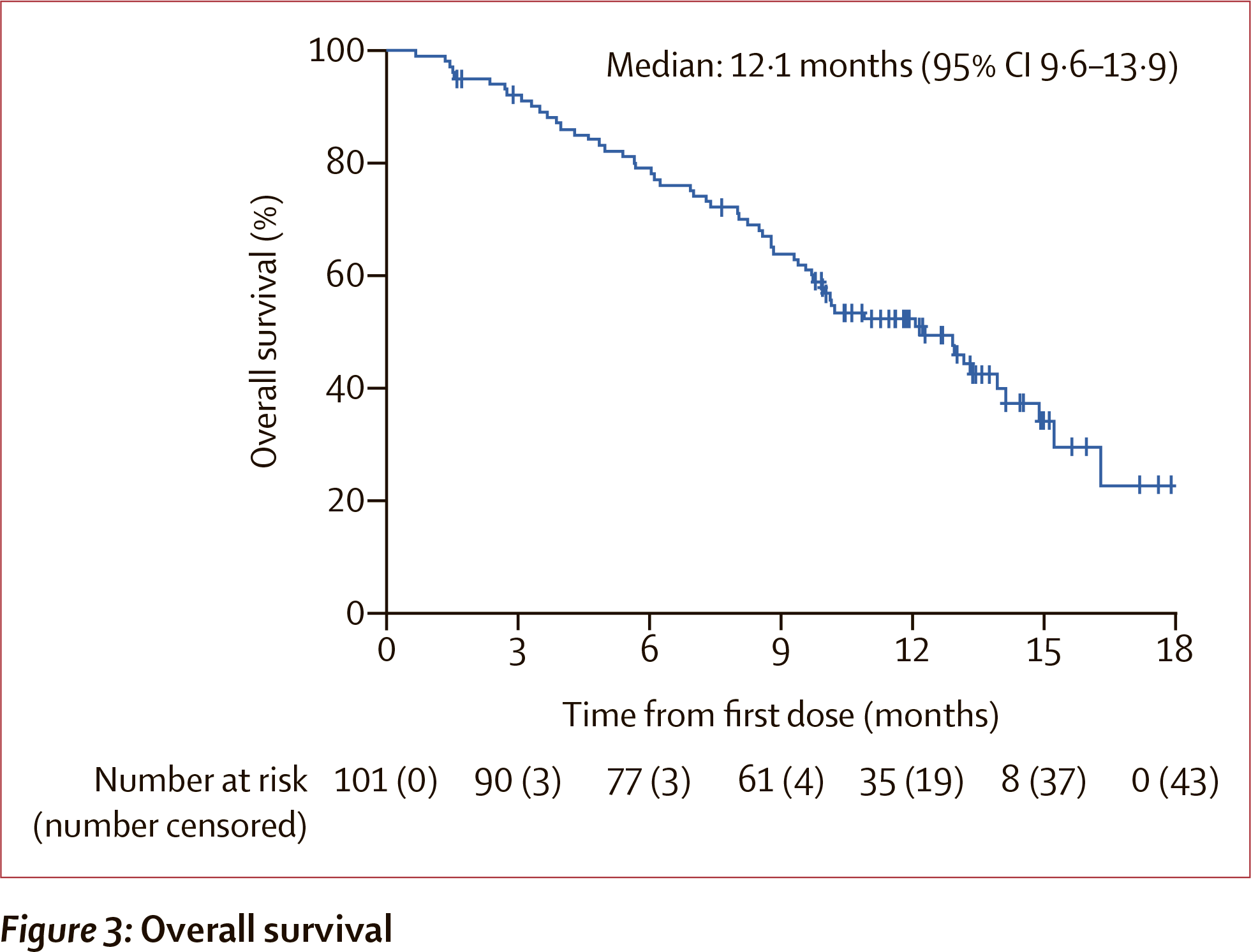
Median overall survival was recorded at 12.1 months (95% CI: 9.6–13.9). At least 6 months, 79% (95% CI: 69–86) of subjects survived; at least 12 months, 51% (95% CI: 41–61) survived.
Median progression-free survival was 4.2 months (95% CI: 3.0–4.4).
The prescribing information of Tivdak comes with black box warning about the risk of changes in the corneal epithelium and conjunctiva that may lead to visual impairment (including vision loss) and corneal ulceration. Regular ophthalmologic examinations, proper premedication, and drug discontinuation or dose reduction are recommended.
Common adverse events reported during tisotumab vedotin include: hemoglobin decreased (in 52% of patients), fatigue (50%), lymphocytes decreased (42%), nausea (41%), peripheral neuropathy (39%), alopecia (39%), epistaxis (39%), conjunctival adverse reactions (37%), hemorrhage (32%), leukocytes decreased (30%).
Because of the adverse events, 13% of the subjects discontinued treatment completely, 47% temporarily interrupted treatment, and 23% reduced the dose of Tivdak.
Tisotumab Vedotin: What’s Next
According to industry forecasts, peak sales of Tivdak will exceed $600 million, and that will happen by 2026.
Seagen and Genmab continue their clinical review of tisotumab vedotin, hoping to expand the range of therapeutic indications for Tivdak:
- innovaTV 301 (NCT04697628) phase 3: second- or third-line therapy for recurrent or metastatic cervical cancer — monotherapy with tisotumab vedotin versus chemotherapies (topotecan, vinorelbine, gemcitabine, irinotecan or pemetrexed).
- innovaTV 205 (NCT03786081) phase 1/2: previously untreated or already undergoing systemic therapy (no more than two lines) for recurrent or stage IVB cervical cancer — monotherapy with tisotumab vedotin or its combination with bevacizumab, pembrolizumab, or carboplatin.
- innovaTV 206 (NCT03913741) phase 1/2: locally advanced or metastatic solid tumors that have progressed after standard treatment — monotherapy with tisotumab vedotin.
- innovaTV 207 (NCT03485209) phase 2: relapsed, locally-advanced or metastatic colorectal cancer, pancreatic exocrine adenocarcinoma, squamous non-small cell lung cancer (NSCLC), or squamous cell carcinoma of head and neck (SCCHN) after systemic therapy — monotherapy with tisotumab vedotin or its combination with pembrolizumab and carboplatin (or cisplatin).
- innovaTV 208 (NCT03657043) phase 2: previously treated platinum-resistant epithelial ovarian cancer, primary peritoneal cancer, or fallopian tube cancer — monotherapy with tisotumab vedotin.
Extras
Tivdak (tisotumab vedotin). Prescribing information. U.S. [PDF]
Efficacy and safety of tisotumab vedotin in previously treated recurrent or metastatic cervical cancer (innovaTV 204/GOG-3023/ENGOT-cx6): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2021 May;22(5):609-619. [source]