Highlights
The combination of Tecentriq (atezolizumab) and Avastin (bevacizumab) proposed by Roche is used in the first-line treatment of unresectable or metastatic hepatocellular carcinoma (HCC) that has not yet received systemic therapy.
In all key clinical measures, this drug combination is more effective than the standard first-line liver cancer therapy with Nexavar (sorafenib), a multikinase inhibitor by Bayer. The immunotherapy approach also outperformed the similar multikinase inhibitor Lenvima (lenvatinib) promoted by Eisai and Merck & Co. and with comparable efficacy to sorafenib.
Tecentriq with Avastin is a powerful new pharmacotherapy for liver cancer, which in the past dozen years has succeeded in becoming the first life-prolonging one. And it is more than in demand, because hepatocellular carcinoma, being an incredibly difficult cancer to treat, is characterized by the highest mortality rate.
Liver Cancer: Some Features
Liver cancer, which is represented by hepatocellular carcinoma in 90% of cases, is the fifth most common cancer worldwide and the third most lethal. The incidence of liver cancer and mortality rates vary geographically due to differences in epidemiological factors and therapeutic approaches. For example, the incidence of liver cancer in Southeast Asia is nearly four times higher than in Northern Europe.
Liver cancer is still one of the most difficult to treat because most cases are diagnosed virtually by accident during ultrasound, CT and/or MRI scans, when it has already reached an advanced, unresectable stage, due to its generally asymptomatic course. This is why periodic screening is in demand, especially in the high-risk population of patients with chronic liver damage due to alcoholism, chronic viral hepatitis B or C, biliary cholangitis, nonalcoholic fatty liver disease (NAFLD) and/or nonalcoholic steatohepatitis (NASH) with metabolic syndrome or diabetes mellitus.
Treatment of early-stage hepatocellular carcinoma involves surgical resection of the liver or liver transplantation. If these interventions, which can potentially cure the disease, are not suitable, locoregional therapy is prescribed.
Locoregional therapy is represented by three groups of non-surgical interventions:
- ablation: radiofrequency ablation (RFA), microwave ablation, percutaneous ethanol injections (PEI) or acetic acid injections, laser ablation, high-intensity focused ultrasound (HIFU), cryoablation, irreversible electroporation (IRE)
- embolization: transarterial embolization (TAE), transarterial chemoembolization (TACE), transarterial radioembolization (TARE)
- external beam radiation therapy (EBRT): stereotactic body radiation therapy (SBRT), intensity-modulated radiation therapy (IMRT), 3-dimensional conformal radiation therapy (3D-CRT), proton beam irradiation (PBI).
Treatment of unresectable, inoperable or metastatic hepatocellular carcinoma is generally limited to either participation in clinical trials or pharmacotherapy. Among the systemic drugs used are: chemotherapy drugs; the tyrosine kinase inhibitors (TKIs) Nexavar (sorafenib), Lenvima (lenvatinib), Stivarga (regorafenib), and Cabometyx (cabozantinib); the vascular endothelial growth factor receptor 2 (VEGFR2) antagonist Cyramza (ramucirumab); vascular endothelial growth factor A (VEGF-A) inhibitor Avastin (bevacizumab); programmed cell death protein 1 (PD-1) blockers Opdivo (nivolumab) and Keytruda (pembrolizumab).
In late May 2019, Roche, through its Genentech division, proposed a revolutionary way to treat liver cancer using Tecentriq, a programmed death-ligand 1 (PD-L1) blocker, in combination with Avastin. The combination was so effective that it easily displaced Nexavar, which had held the monopoly on the first-line therapy for unresectable hepatocellular carcinoma for nearly 12 years.
It is possible that the pharma industry will develop improved immunotherapies for liver cancer in the future, but for now, Tecentriq with Avastin is the best therapeutic choice for unresectable hepatocellular carcinoma.
Immunotherapy Against Liver Cancer: Mechanism of Action
PD-(L)1 blockers have started a revolution in cancer immunotherapy: removing the “brakes” from the immune system has proven suitable for therapy of almost any solid tumor. But not in the case of liver cancer. Yes, monotherapy with Opdivo or Keytruda, PD-1 blockers by Bristol-Myers Squibb and Merck & Co., gave a 15%–20% response to treatment during first- and second-line therapy for hepatocellular carcinoma, although it did not significantly prolong overall survival.
There are many ways in which tumor cells escape immunological surveillance. Overexpression of vascular endothelial growth factor (VEGF) seen in hepatocellular carcinoma is thought to activate immunosuppression by myeloid-derived suppressor cells (MDSCs) and regulatory T cells. If bevacizumab, a VEGF-A inhibitor, is added to the PD-L1 blocker atezolizumab, one would expect inhibition of immunosuppression followed by stimulation of tumor infiltration by T cells and priming and activation of T-cell responses against tumor antigens. This is what happened.

A separate analysis reinforced the confidence in the mechanistic hypothesis that adding VEGF blockade to immune checkpoint inhibitors was justified. It was found that the chances of therapeutic response and prolonged progression-free survival increase with high PD-L1 expression and T-effector signaling (CXCL9, PRF1, GZMB) and, in contrast, fall with Notch activation. In view of the fact that VEGF/VEGFR signaling in hepatocellular carcinoma promotes immunosuppression in addition to angiogenesis, high expression levels of VEGFR2, T-regulatory signatures (CCR8, BATF, CTSC, TNFRSF4, FOXP3, TNFRSF18, IKZF2, IL2RA), myeloid inflammatory signatures (CXCL1, CXCL2, CXCL3, CXCL8, IL6, PTGS1) and MDSC-like TREM1 expression are all possibly associated with improved clinical outcomes.
Tecentriq With Avastin for Treatment of Unresectable Liver Cancer: Efficacy and Safety
The IMbrave150 (NCT03434379) phase 3 (randomized, open-label, multicenter, international) clinical trial enrolled adult patients (n=501) with locally advanced or metastatic and/or unresectable hepatocellular carcinoma (HCC) not previously treated systemically.
Participants were treated with either atezolizumab with bevacizumab or sorafenib until disease progression or unacceptable toxicity. Because of adverse reactions, subjects could withdraw from atezolizumab or bevacizumab and continue therapy with one of the remaining drugs.
Main Results
At a median follow-up of 8.6 months, median overall survival (OS) was not achieved in the Tecentriq group with Avastin — versus 13.2 months (95% CI: 10.4–NE) in the Nexavar group. Experimental treatment provided a 42% reduction in risk of death: hazard ratio (HR) 0.58 (95% CI: 0.42–0.79); p=0.0006.
The combination of atezolizumab with bevacizumab endowed patients with significantly higher odds of remaining alive at 6 and 12 months: 84.8% (95% CI: 80.9–88.7) and 67.2% (95% CI: 61.3–73.1), respectively — vs. 72.2% (95% CI: 65.1–79.4) and 54.6% (95% CI: 45.2–64.0).

The median progression-free survival (PFS) came out to 6.8 months (95% CI: 5.8–8.3) — vs. 4.3 months (95% CI: 4.0–5.6). The risk of disease progression or death was reduced by 41%: HR 0.59 (95% CI: 0.47–0.76); p<0.0001. The six-month PFS rate was fair for 54.5% of patients — vs. 37.2%.

The overall response rate (ORR), according to the RECIST 1.1 criteria modified for hepatocellular carcinoma, was 33.2% (95% CI: 28.1–38.6) with the combination of Tecentriq and Avastin — vs. 13.3% (95% CI: 8.4–19.6) in the Nexavar group (p<0.001). Meanwhile, complete response (CR) and partial response (PR) were noted for 10.2% and 23.1% of subjects in the combination treatment group — vs. 1.9% and 11.4% in the control group.

The duration of response (DoR) with atezolizumab with bevacizumab has not yet reached the median value, ranging from 1.3+ to 13.4+ months — vs. a median of 6.3 months (95% CI: 4.9–NE) with sorafenib, for which the range was 1.4+ to 9.1+ months.
Although the time to response (TTR) in the experimental and comparison groups was similar, the width and depth of response to treatment was significantly better among those receiving immuno-oncology therapy. In the vast majority of those who showed a complete response, it lasted for more than 6 months, with a median still unestablished. Moreover, emergence into remission was possible regardless of poor prognostic factors or etiology of hepatocellular carcinoma.
Neither Tecentriq with Avastin nor Nexavar is safe, because they all have a significant and broad spectrum of adverse reactions.
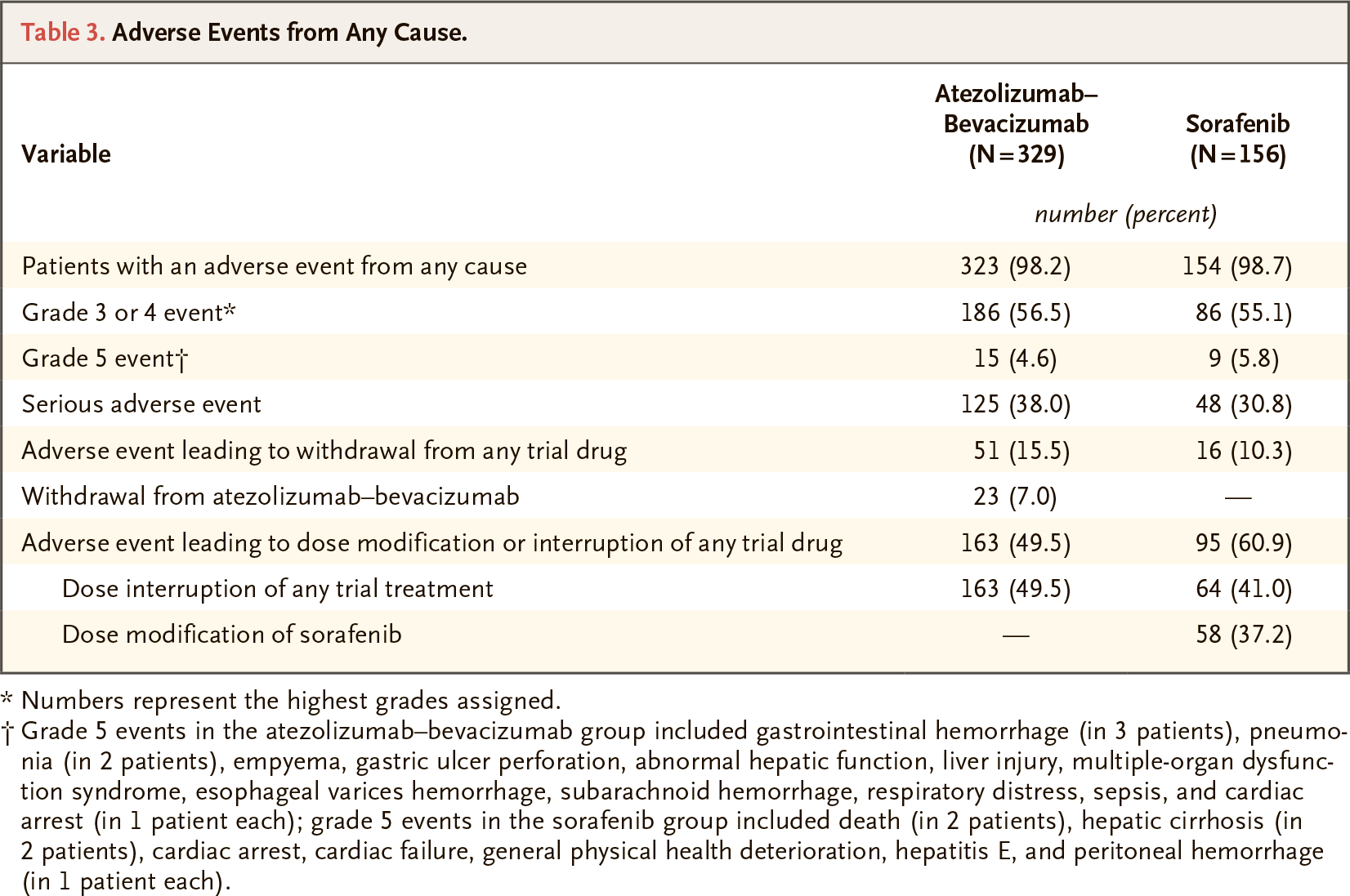
One of the safety concerns with atezolizumab and bevacizumab in hepatocellular carcinoma is the adverse reactions associated with the specific mechanism of action of these drugs.
Thus, the use of PD-(L)1 blockers is often accompanied by negative events due to immune system activation manifested by dermatological, gastrointestinal (GI) and endocrine events. VEGF inhibitors carry risks of bleeding, with bleeding from the upper GI tract a common and life-threatening complication inherent in hepatocellular carcinoma, especially in the presence of cirrhosis.
Roche, however, has assured that such adverse reactions, well known with Tecentriq and Avastin, are manageable.
Long-Term Follow-Up Results
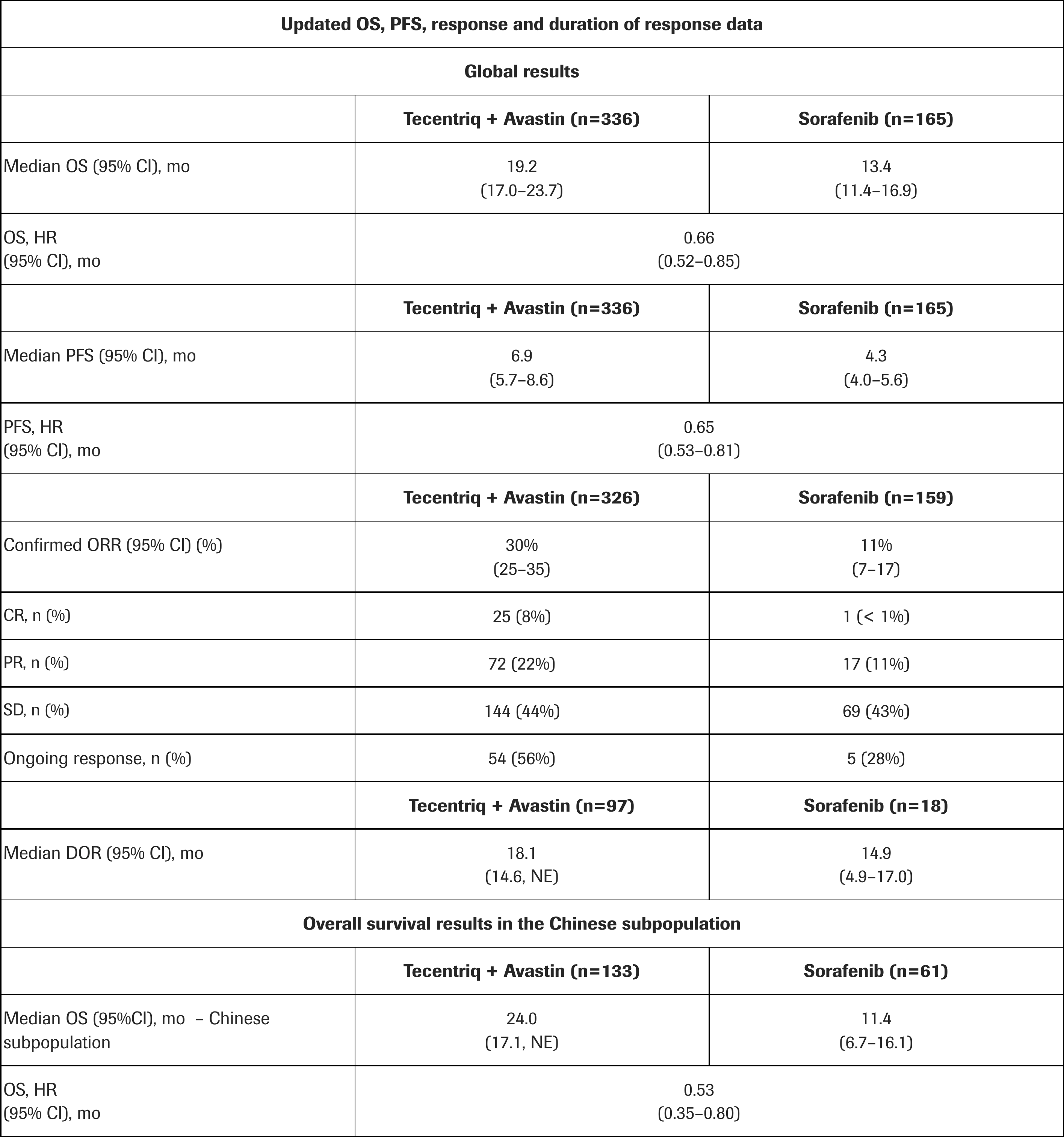
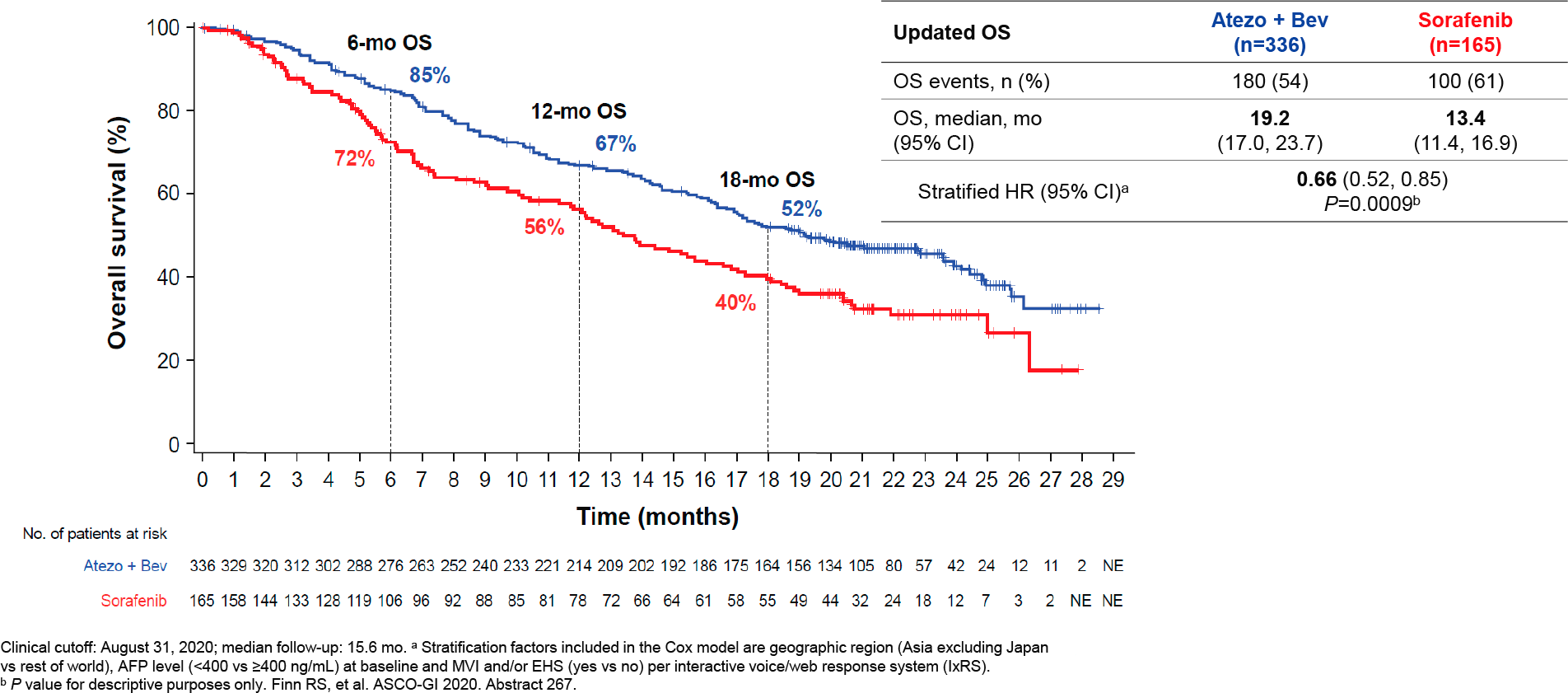
At a median follow-up of 15.6 months, first-line treatment of hepatocellular carcinoma with Tecentriq and Avastin was found to produce a median overall survival (OS) of 19.2 months (95% CI: 17.0–23.7) — versus 13.4 months (95% CI: 11.4–16.9) with Nexavar. Atezolizumab with bevacizumab reduced the risk of death by 34%: HR 0.66 (95% CI: 0.52–0.85; p=0.0009).
- In the Chinese patient population (n=194), these rates were even better. The median OS was 24.0 months (95% CI: 17.1–NE) — vs. 11.4 months (95% CI: 6.7–16.1); HR 0.53 (95% CI: 0.35–0.80).
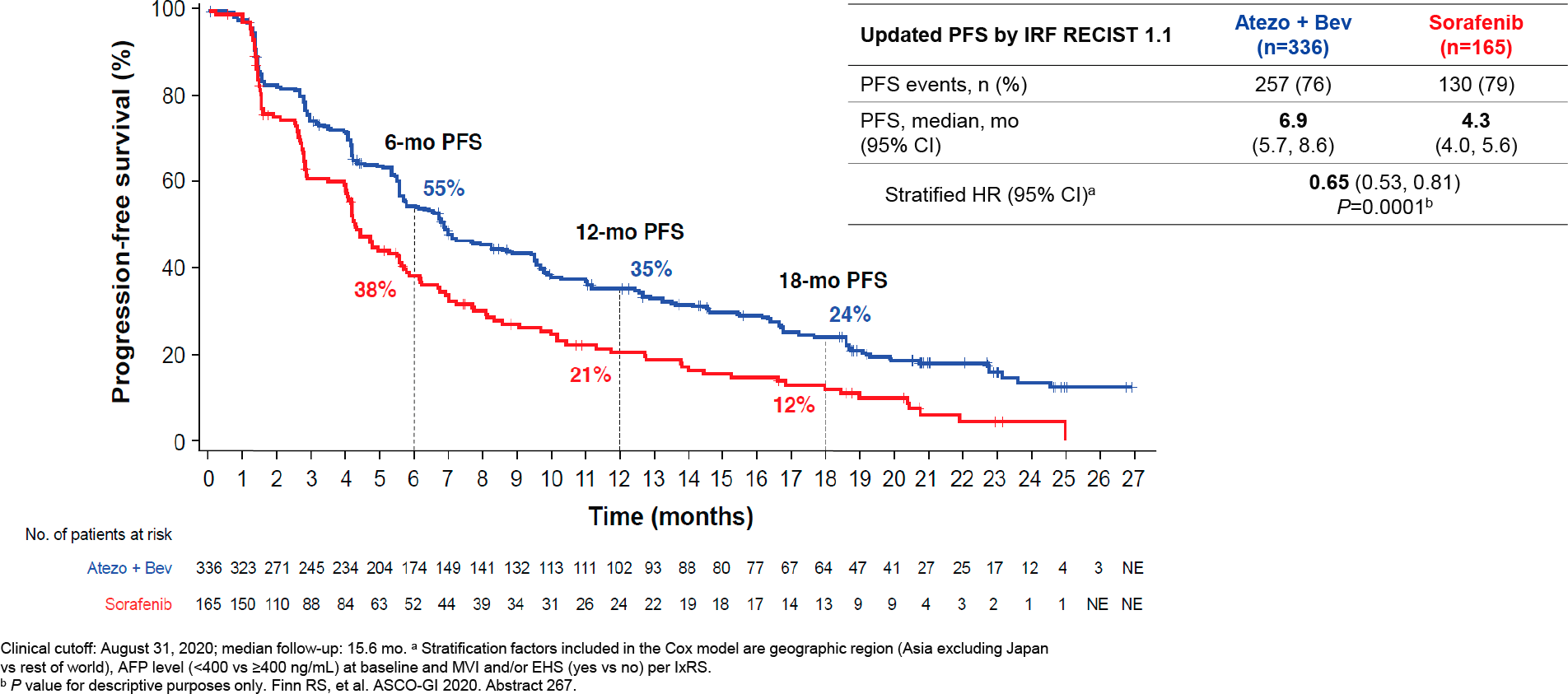
Median progression-free survival (PFS) was 6.9 months (95% CI: 5.7–8.6) — vs. 4.3 months (95% CI: 4.0–5.6). The reduction in risk of disease progression or death realized by Tecentriq with Avastin was 35%: HR 0.65 (95% CI: 0.53–0.81; p=0.0001).
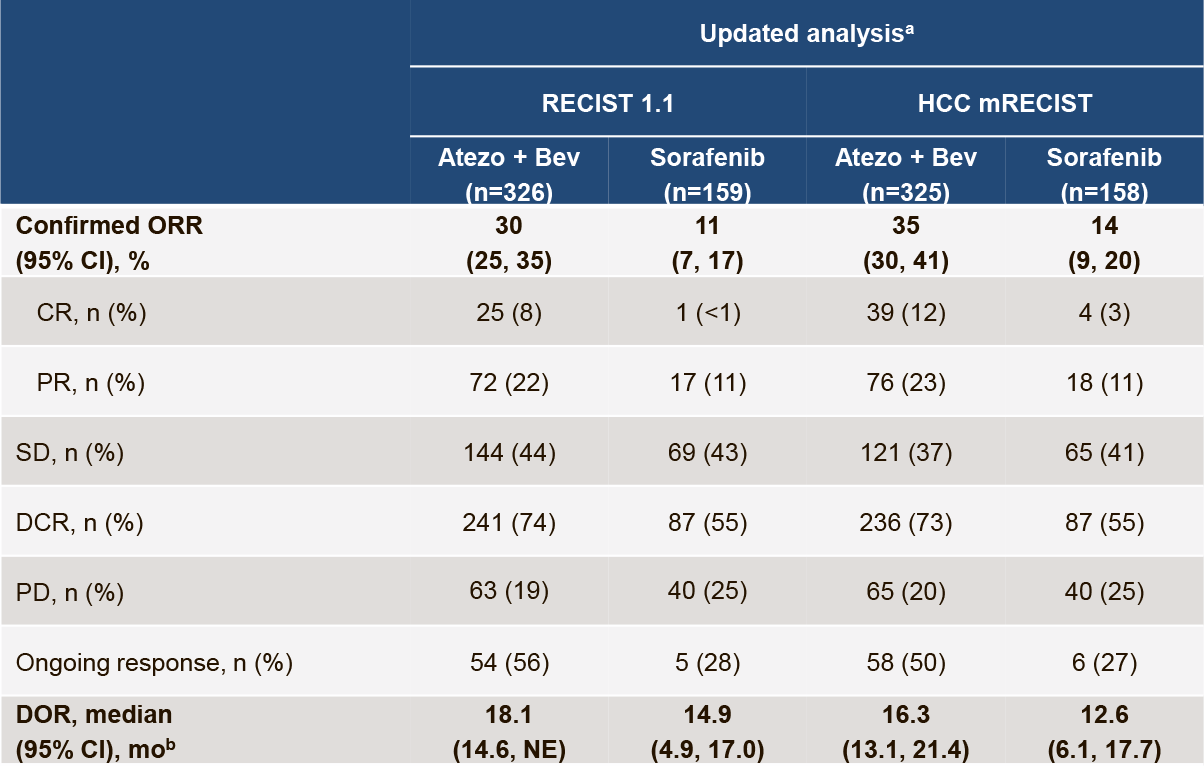
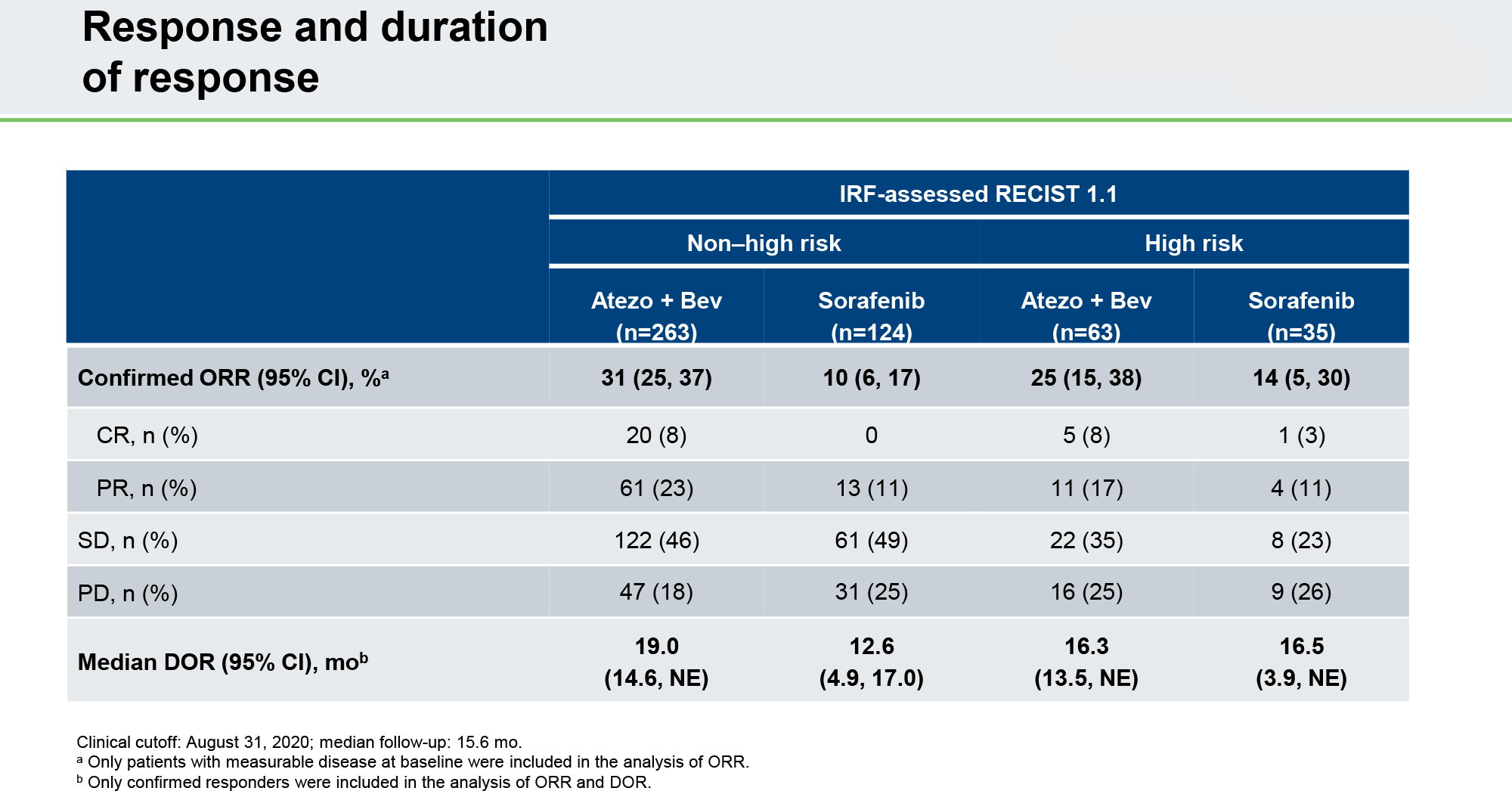
Overall response rate (ORR) was recorded at 30% (95% CI: 25–35), including 8% complete responses (CR) and 22% partial responses (PR) — vs. 11% (95% CI: 7–17), including CR < 1% and PR 11%.
The median duration of response (DoR) was 18.1 months (95% CI: 14.6–NE) — vs. 14.9 months (95% CI: 4.9–17.0).
Prior Locoregional Treatment of Liver Cancer
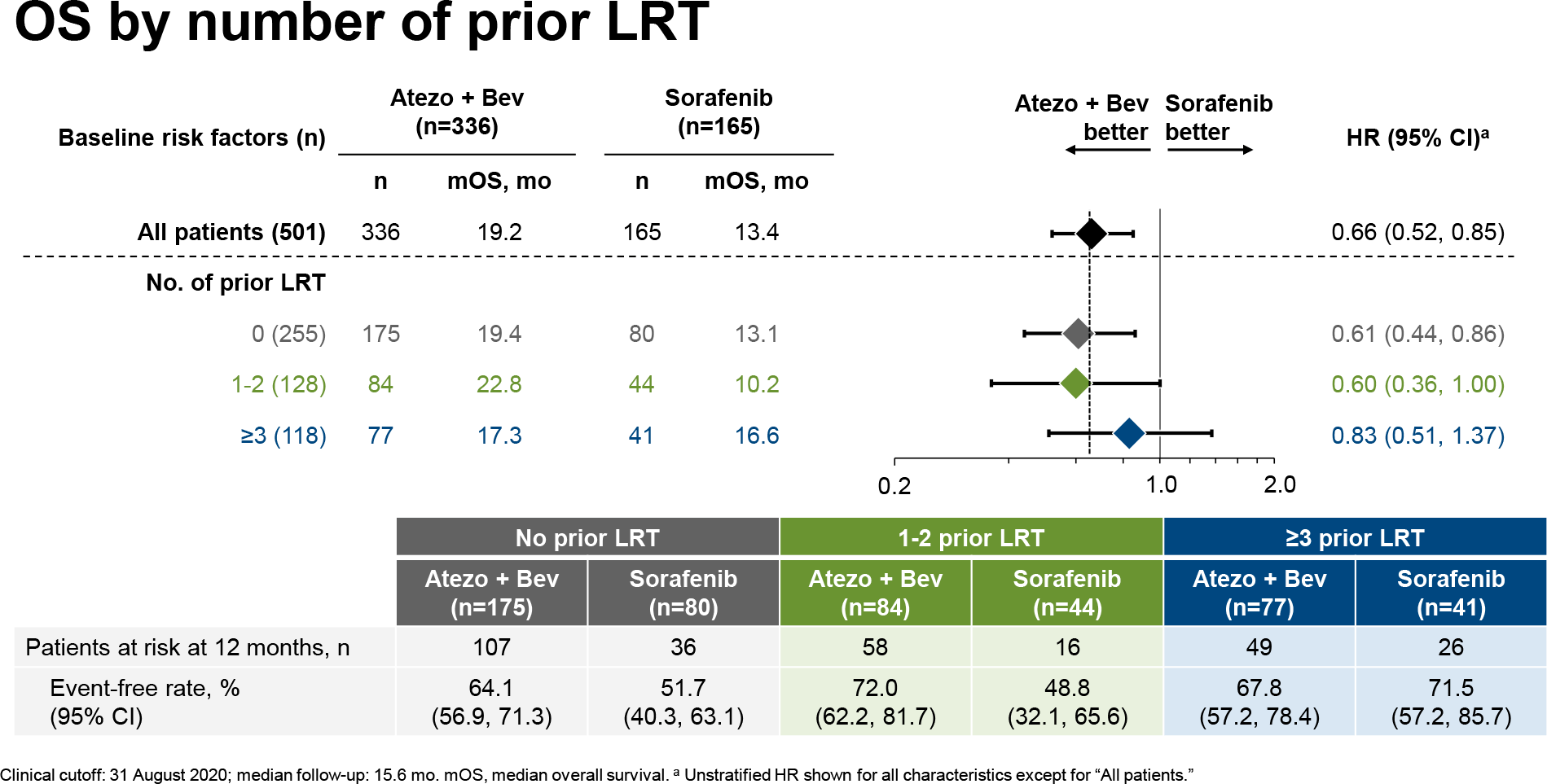
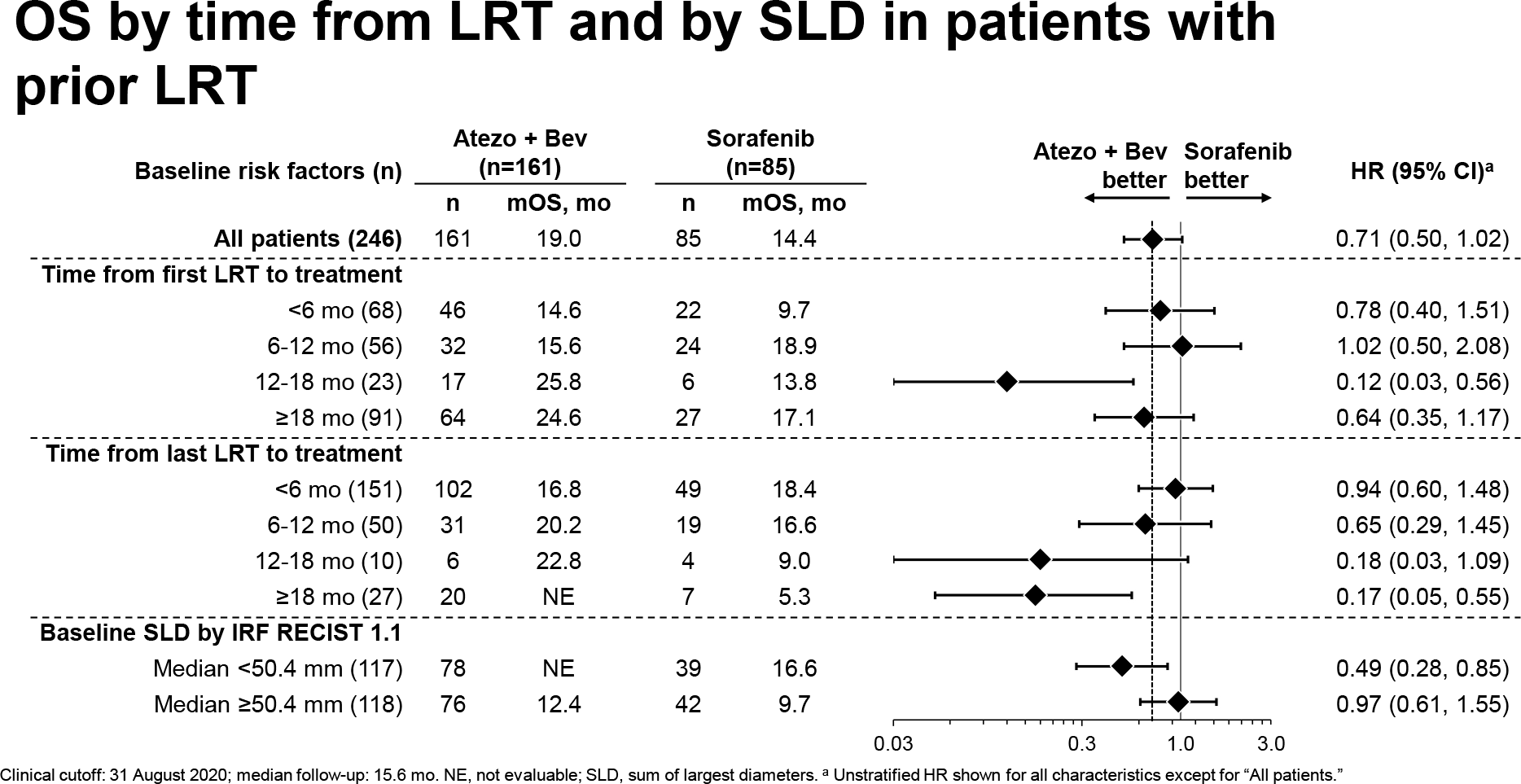
The prolongation of survival provided by Tecentriq with Avastin compared with Nexavar in first-line therapy for hepatocellular carcinoma was noted regardless of whether patients had previously received locoregional treatment. However, the immuno-oncologic combination seemed to be of greater benefit with one or two lines of locoregional therapy (LRT) than with three or more.
Thus, median overall survival (OS) among those who had previously received one or two lines of LRT was 22.8 months — versus 17.3 months among those who received three or more such lines: HR 0.60 (95% CI: 0.36–1.00) and 0.83 (95% CI: 0.51–1.37).
Patients who benefited most from OS were those for whom either the time since the first LRT before systemic treatment fell within the 12–18 months range (HR 0.12 [95% CI: 0.03–0.56]) or the time since the last LRT before systemic treatment fell within the 18 months or more range (HR 0.17 [95% CI: 0.05–0.55]).
Treating Liver Cancer in High-Risk Patients
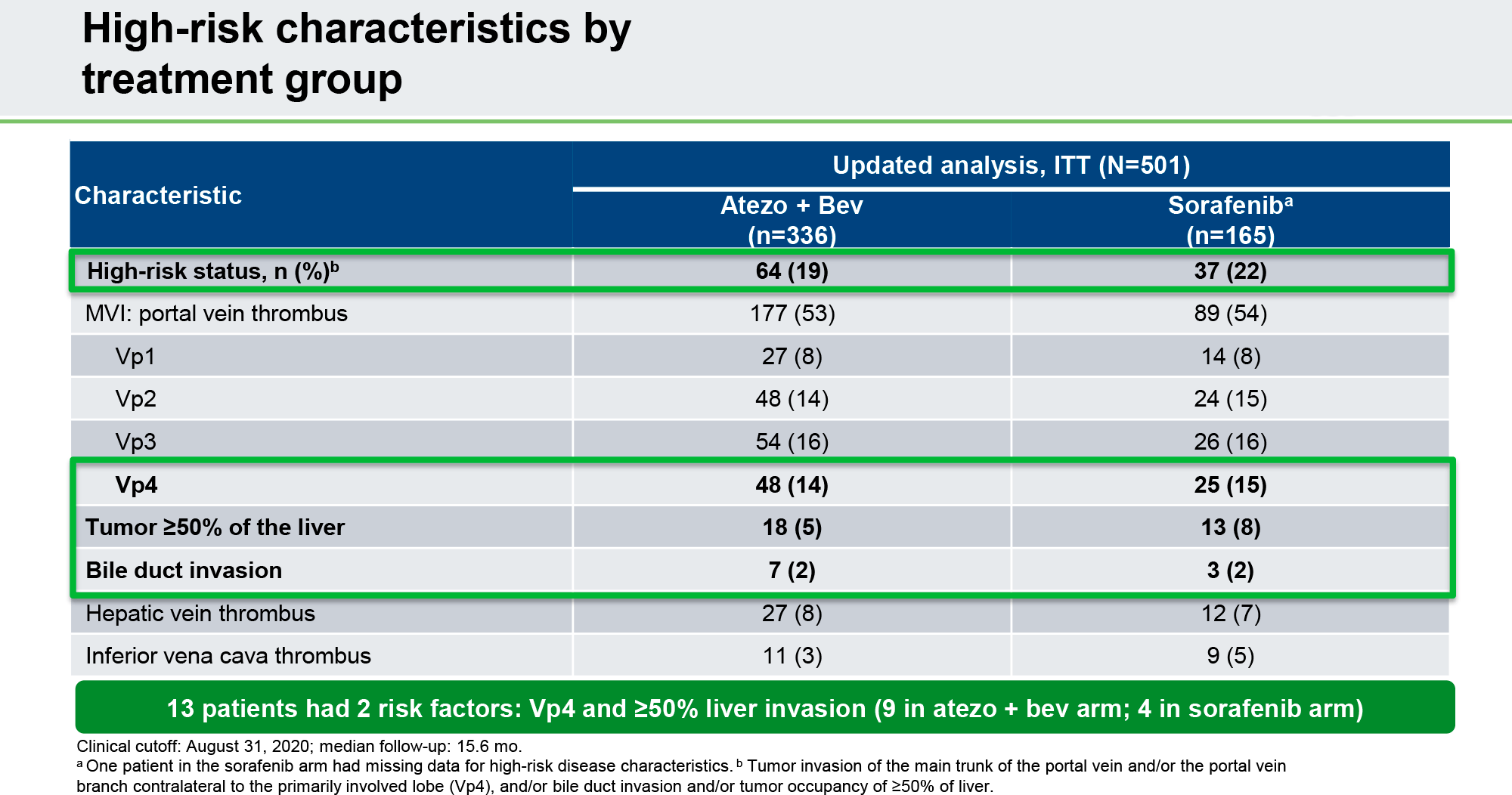
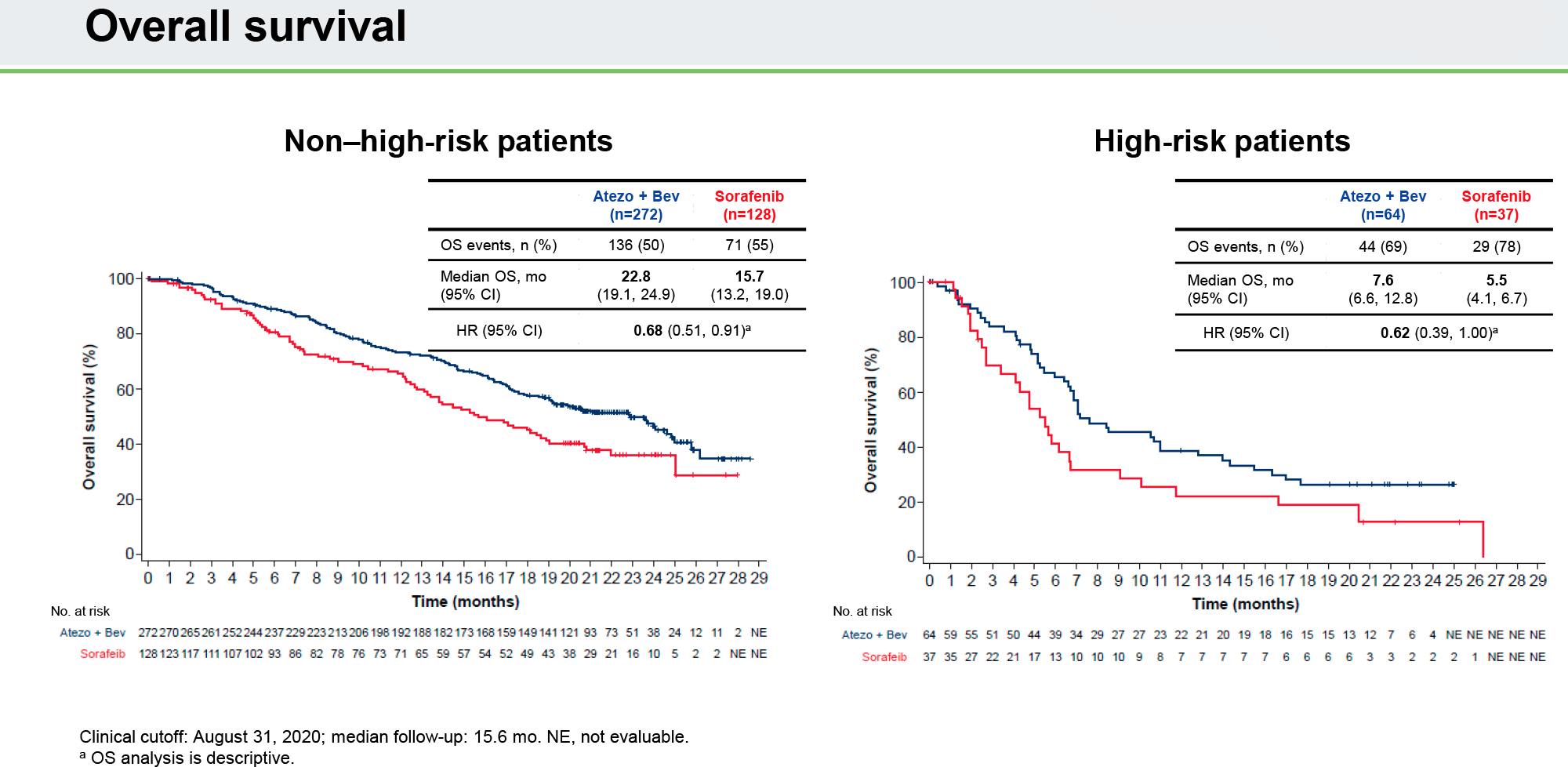
Tecentriq with Avastin maintained their superior therapeutic efficacy to Nexavar in the first-line treatment of liver cancer regardless of patients’ risk status. High-risk patients, however, were marked, as one would expect, by a clear numerical drop in all measures of treatment efficacy.
- High risk refers to the presence of tumor invasion of the main trunk of the portal vein and/or the portal vein branch contralateral to the primiraly involved liver lobe (Vp4), and/or bile duct invasion and/or tumor occupancy of ≥ 50% of the liver.
For example, whereas among patients without high risk the median overall survival (OS) was 22.8 months (95% CI: 19.1–24.9) and 15.7 months (95% CI: 13.2–19.0) in the atezolizumab with bevacizumab and sorafenib groups, respectively, it decreased to 7.6 months (95% CI: 6.6–12.8) and 5.5 months (95% CI: 4.1–6.7) among high-risk patients. In any case, the use of Tecentriq with Avastin outperformed Nexavar: HR 0.68 (95% CI: 0.51–0.91) and 0.62 (95% CI: 0.39–1.00).
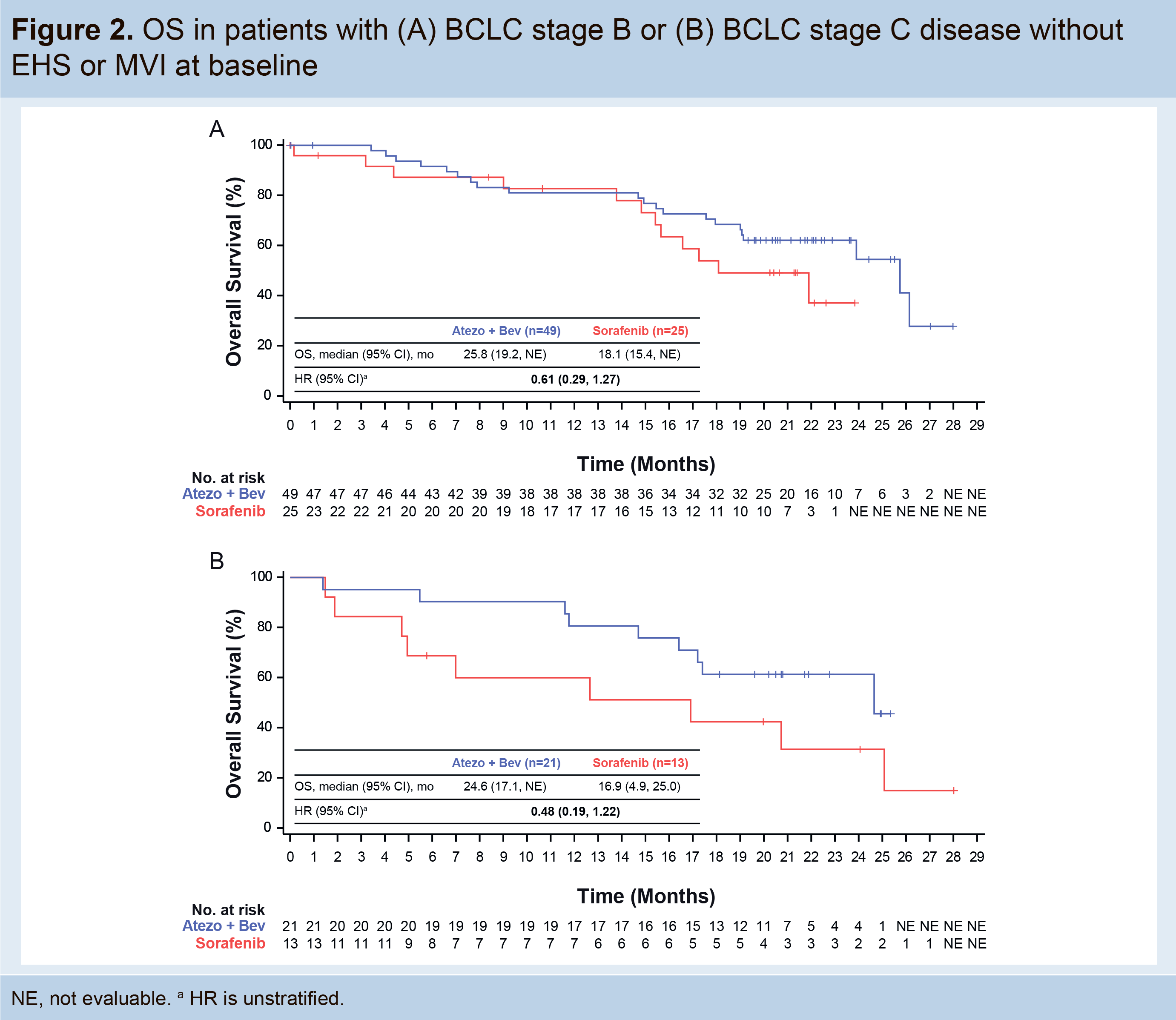
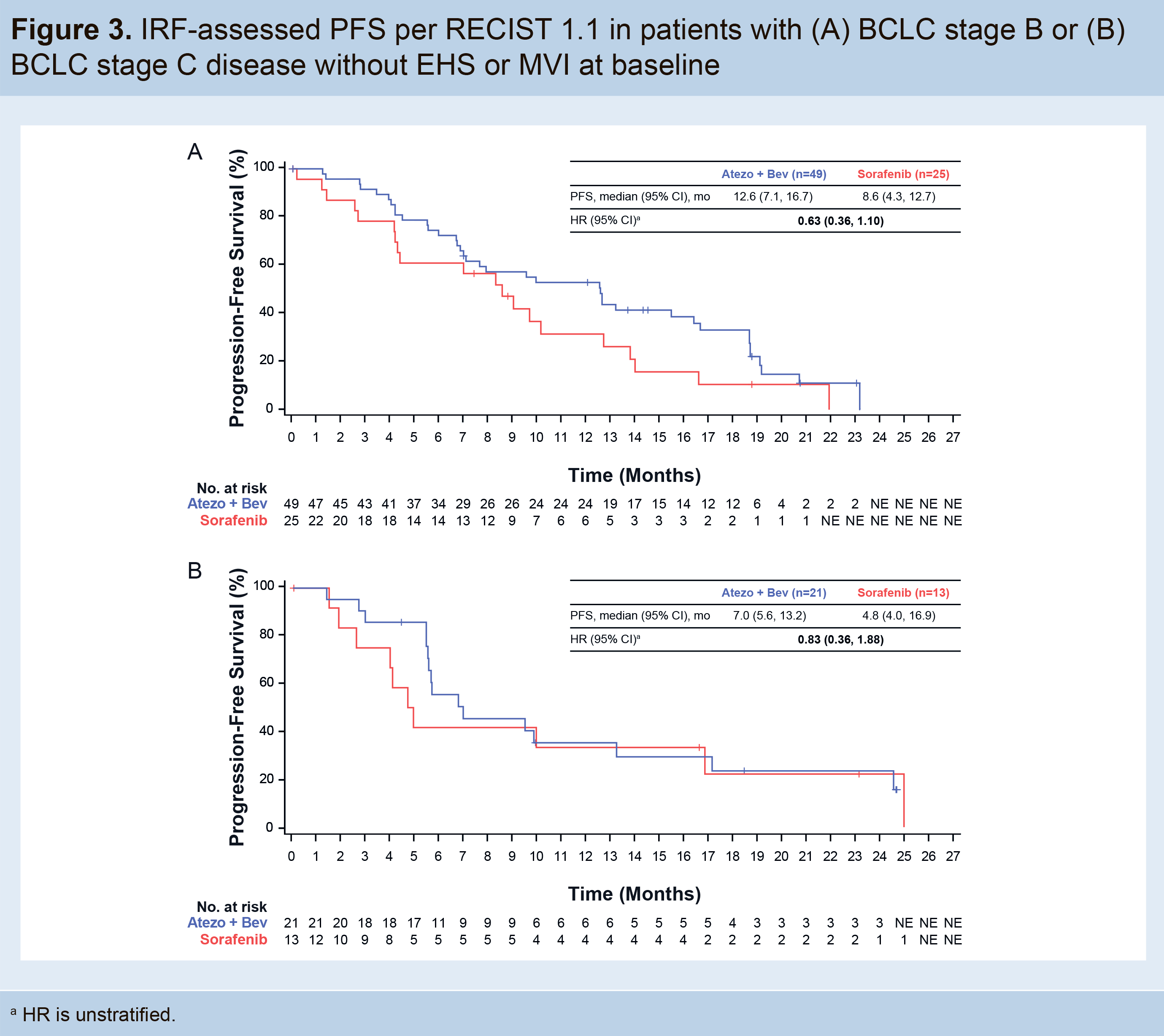
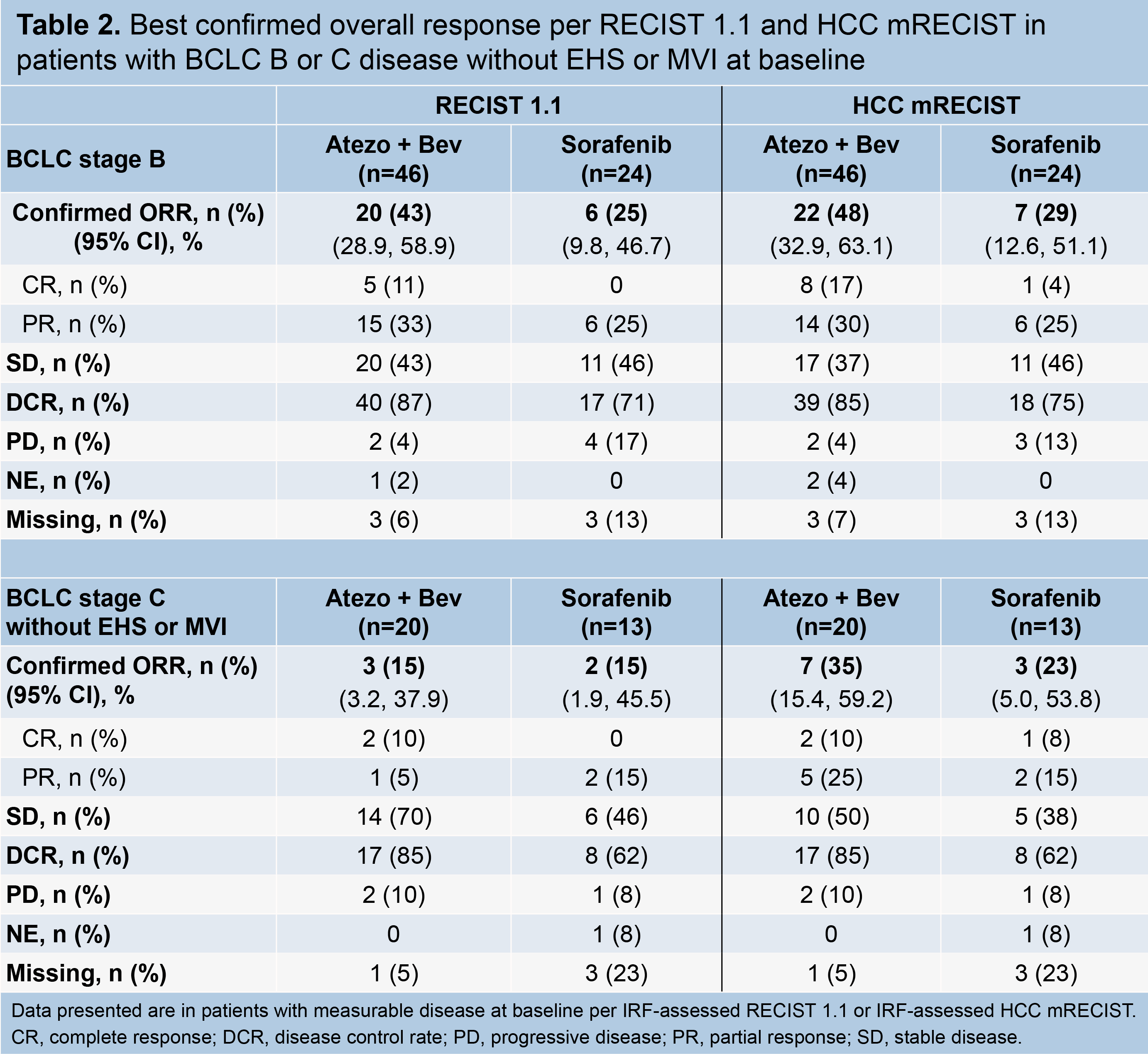
Treating Liver Cancer in Low-Risk Patients
When it comes to low-risk patients, first-line treatment for hepatocellular carcinoma with Tecentriq and Avastin has similarly outperformed Nexavar therapy.
- Low risk refers to the absence of extrahepatic spread (EHS) or macrovascular invasion (MVI).
For example, median overall survival (OS) among low-risk patients with stage B or C liver cancer, according to the Barcelona Clinic Liver Cancer (BCLC) staging system, came out to 25.8 months (95% CI: 19.2–NE) and 24.6 months (95% CI: 17.1–NE) with atezolizumab and bevacizumab — versus 18.1 months (95% CI: 15.4–NE) and 16.9 months (95% CI: 4.9–25.0) with sorafenib: HR 0.61 (95% CI: 0.29–1.27) and 0.48 (95% CI: 0.19–1.22).
Treatment of Hepatocellular Carcinoma After Disease Progression
Roche has found that it is reasonable to continue treatment with Tecentriq with (or without) Avastin for hepatocellular carcinoma even after it has progressed. That said, it is appropriate to stop such ongoing therapy when clinical benefit is lost, not when radiographic progression has occurred.
Thus, the median overall survival (OS) for continued treatment after liver cancer progression was 14.5 months (95% CI: 11.5–16.7) during administration of atezolizumab with (or without) bevacizumab. The 12-month survival rate came out to 59.1% (95% CI: 49.6–68.6).
The median OS with other drugs, including sorafenib and lenvatinib, was significantly shorter at 6.8 months (95% CI: 4.9–11.5) and the 12-month survival rate was 35.6% (95% CI: 22.6–48.6).
If hepatocellular carcinoma was left untreated after progression, the median OS was 2.0 months (95% CI: 1.6–3.0) and the 12-month survival rate was 6.0% (95% CI: 0.0–13.8).

Biomarker: Circulating Tumor DNA (ctDNA)
To help the physician community, Roche has shown that personalized, noninvasive tests detecting circulating tumor DNA (ctDNA) are appropriate in the task of tracking the clinical effectiveness of hepatocellular carcinoma treatment.
The role of ctDNA as a promising biomarker whose level correlates with disease severity has been demonstrated. Thus, if the initial level of ctDNA before the start of liver cancer treatment was high, disease progression was observed in a shorter period of time. In contrast, if the ctDNA level fell (or even disappeared) with treatment of hepatocellular carcinoma, the overall response rate (ORR), overall survival (OS), and progression-free survival (PFS) improved.
Biomarker: Alpha-Fetoprotein (AFP)
Alpha-fetoprotein (AFP) is a glycoprotein produced by the liver during the early embryonic stage of development and in certain cancers, including hepatocellular carcinoma, hepatoblastoma, non-seminomatous ovarian and testicular germ cell tumors. Normal AFP levels should be less than 10 ng/mL. In approximately half of all cases of advanced hepatocellular carcinoma, high levels of AFP are detected; such patients have a poor prognosis. This is due to the fact that increased AFP concentration correlates with increased expression of vascular endothelial growth factor receptors (VEGFRs) responsible for tumor angiogenesis.
Roche assessed the correlation of changes in AFP levels with response to hepatocellular carcinoma treatment with Tecentriq and Avastin among patients with baseline AFP levels > 20 ng/mL. It was found that a decrease of ≥ 75% or an increase of ≤ 10% in AFP levels measured 6 weeks after initiation of therapy can serve as an acceptable prognostic biomarker to identify patients who are likely to respond to treatment and/or give a longer overall survival (OS) and progression-free survival (PFS).
Cost-Effectiveness of Liver Cancer Treatment
According to the cost-effectiveness assessment of the use of Tecentriq with Avastin for first-line therapy of liver cancer, this combination falls within the range of acceptable use of financial resources of the health care system. At least that is the conclusion reached after analyzing data in Italy.
Tecentriq With Avastin: Best Hepatocellular Carcinoma Treatment
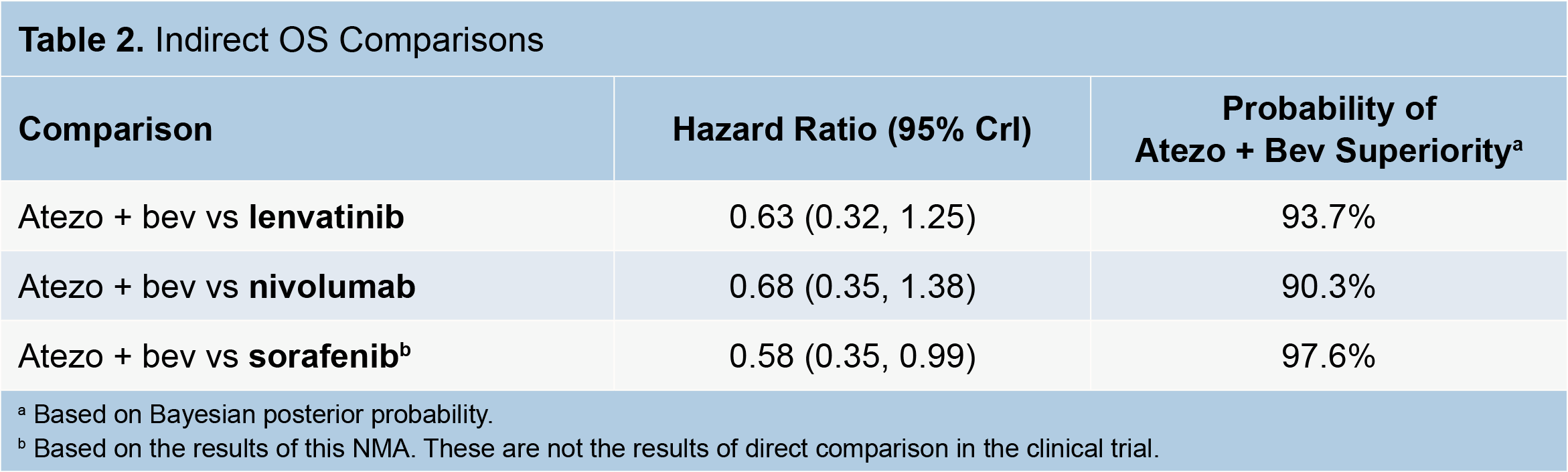
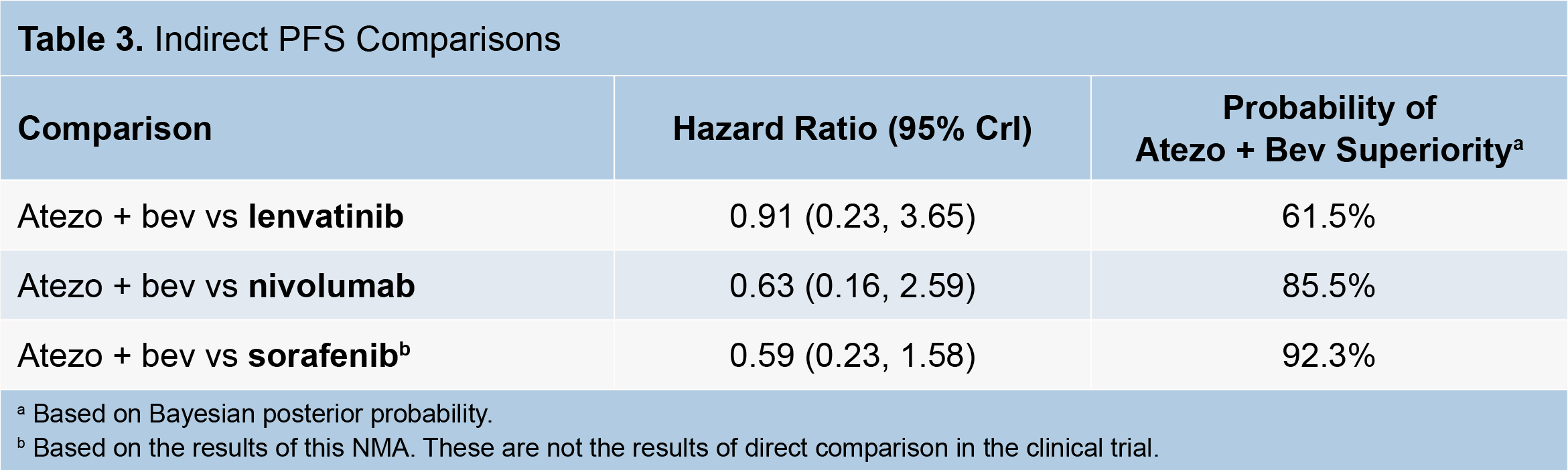
Roche performed a network meta-analysis of the clinical outcomes of Tecentriq with Avastin, Lenvima, and Opdivo compared with standard Nexavar in the first-line therapy of unresectable hepatocellular carcinoma.
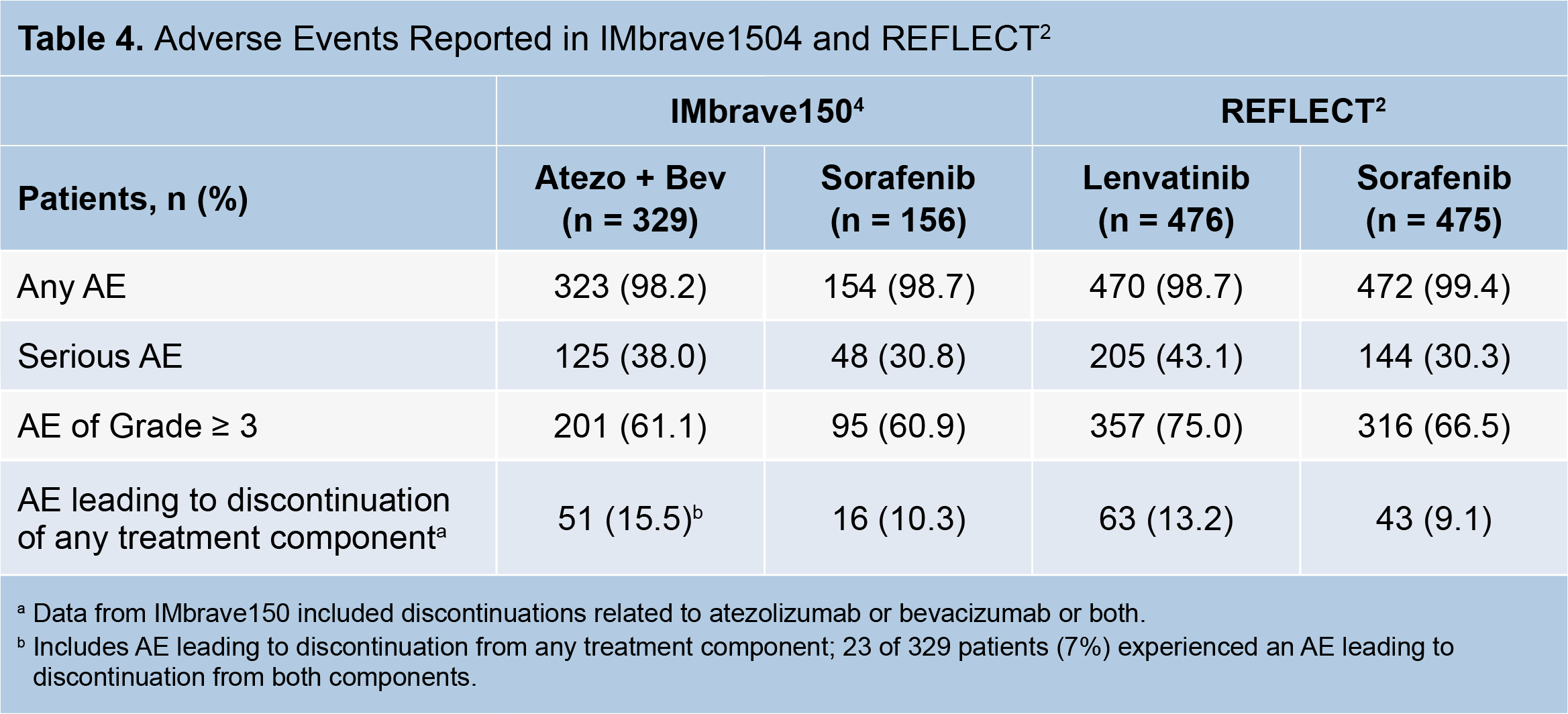
An indirect comparison found that atezolizumab with bevacizumab was more than likely to outperform any of the competing drugs in prolonging both overall survival (OS) and progression-free survival (PFS). At the same time, the incidence of severe adverse reactions was comparable to the notorious and highly toxic sorafenib.
Liver Cancer: All Drugs Are Almost Useless
Roche, which in April 2018 closed a $1.9 billion takeover of Flatiron Health, a startup specializing in developing an electronic medical record system for oncologists, tried to paint a picture of the effectiveness of first-line treatment for hepatocellular carcinoma in practice.
The Swiss pharmaceutical giant did this mainly because the task was to highlight most advantageously the clinical benefits of using Tecentriq with Avastin for liver cancer treatment.
So, information on U.S. patients with hepatocellular carcinoma at any stage diagnosed between January 2011 and December 2018 was extracted from the Flatiron database. The information was grouped according to the eight types of first-line therapy administered, such as liver transplantation, liver resection, radiofrequency ablation (RFA), transarterial chemoembolization (TACE), transarterial radioembolization (TARE) and other locoregional interventions, stereotactic body radiation therapy (SBRT), tyrosine kinase inhibitor (TKI) monotherapy, other systemic treatments including cancer immunotherapy (CIT) or combination therapies.
Baseline characteristics of the patients (n=2134) were that the mean age at diagnosis was 66.1 years, with men accounting for 78%, and chronic hepatitis C was detected in 45% of cases.
If we talk about clinical outcomes in terms of overall survival (OS), as the main criterion of successful treatment of any oncological disease, its median was fixed at the following levels:
- liver transplantation: 75.1 months (95% CI: 55.9–NE)
- liver resection, RFA, SBRT: 47.0 months (95% CI:38.7–58.3)
- TACE, TARE, TAE: 25.4 months (95% CI: 23.1–28.9)
- TKI: 5.0 months (95% CI: 4.5–6.1)
- CIT: 6.7 months (95% CI: 1.1–NE).

Thus, liver transplantation is the most effective way to treat hepatocellular carcinoma, but only 1.6% of patients (n=35/2134) underwent it. This is related both to rather strict requirements for recipient readiness in terms of disease stage and health status, and to the traditional shortage of suitable donor organs.
Liver resection proved to be quite remarkable, prolonging life of patients by a median of 58.3 months (95% CI: 48.4–69.7), first, emphasizing that it is unwise to underestimate its effectiveness, second, testifying that aggressive approaches to treatment of liver cancer are still more justified than more conservative ones.
The most ineffective approach to the treatment of hepatocellular carcinoma was the administration of tyrosine kinase inhibitors, and this despite the fact that one third of patients received them (35.1%; n=751/2134). Such a low success rate of treatment is mainly explained by the advanced stage of the disease, as in 82.1% of cases (n=225/750) it had already reached the metastasis stage, when any existing interventions have drastically reduced the chances of success.

Meanwhile, the disgusting outcomes reported in the clinical practice of tyrosine kinase inhibitors have no explanation for what these drugs promise to doctors and patients. After all, the clinical trials on the basis of which the TKIs have received regulatory approval show much more optimistic prognoses:
- Nexavar (sorafenib), proposed for liver cancer in November 2007, in the SHARP (NCT00105443) phase 3 clinical trial provided a median OS of 10.7 months (95% CI: 9.4–13.3) and PFS of 5.5 months (95% CI: 4.1–6.9) — versus 7.9 months (95% CI: 6.8–9.1) and 2.8 months (95% CI: 2.7–3.9) in the placebo group (HR 0.69 and 0.58).
- Lenvima (lenvatinib), approved against liver cancer in August 2018, in the REFLECT (NCT01761266) phase 3 clinical trial gave a median OS of 13.6 months (95% CI: 12.1–14.9) and PFS of 7.3 months (95% CI: 5.6–7.5) —vs. 12.3 months (95% CI: 10.4–13.9) and 3.6 months (95% CI: 3.6–3.7) in the sorafenib group (HR 0.92 and 0.64).
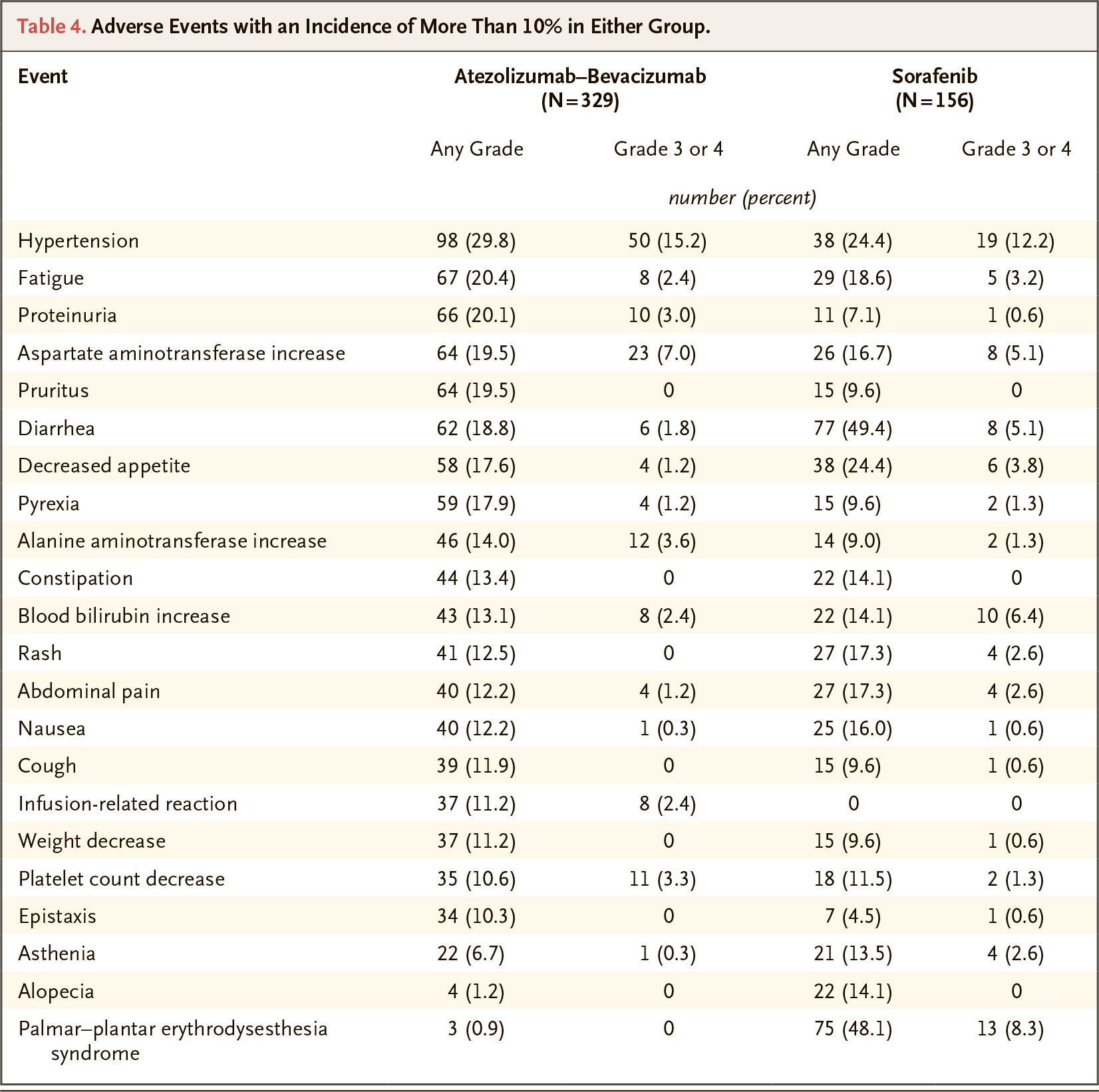
Also not to be forgotten are the frequent adverse side effects of multikinase inhibitors like sorafenib or lenvatinib, such as fatigue, diarrhea, nausea, hypertension, abdominal pain, hand and foot syndrome, itching, and rash.
Obviously, we are dealing with a common situation where the population of patients included in clinical trials does not reflect the characteristics of real patients, not just fully, but at least sufficiently. Pharmaceutical companies have repeatedly been caught in a kind of sleight of hand, where the therapeutic benefits of the new medications being released do not correspond to their effectiveness in reality. And this kind of proclaimed optimism in cancer therapy, which promises hope, is hardly justified — except for those who make money from drugs.
By the way, the lack of effectiveness of sorafenib has been uncovered before. Thus, the median OS from its first-line use was set at 3 months, and even when excluding patient data that could introduce error in the statistical analysis, the overall survival did not exceed 5 months. In general, the OS rate with sorafenib does not differ from that of no treatment at all. There is a similar problem with lenvatinib: its use in practice produces a median OS of about half as much as is claimed in pivotal clinical trial.

Experts believe that the outcomes of sorafenib against hepatocellular carcinoma are significantly influenced by the baseline characteristics of liver function such as ratio of albumin to bilirubin (ALBI), levels of AST, albumin, lactate dehydrogenase (LDH), the patient’s ECOG performance status and age, and etiology of the disease. However, indicators of immune inflammation, alpha-fetoprotein (AFP), and even tumor stage are not significant prognostic factors.
Durvalumab + Tremelimumab: New Effective Immunotherapy for Liver Cancer
Highlights
In mid-January 2022, AstraZeneca revealed how patients with unresectable hepatocellular carcinoma benefit from a cocktail of two immune checkpoint inhibitors.
Imfinzi (durvalumab) with tremelimumab, PD-L1 and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blockers, not only outperformed Nexavar in prolonging life, but also provided a relatively high survival rate in this cancer: a third of liver cancer patients remained alive 3 years after starting treatment.
The immunotherapy combination being developed by AstraZeneca will take its rightful place in the fight against liver cancer. First, effective pharmacological options are decidedly insufficient. Second, the new regimen will suit those patients for whom bevacizumab is contraindicated: especially those patients who have a high risk of bleeding and who cannot undergo endoscopy during the 6 months of therapy.
Details
The ongoing HIMALAYA (NCT03298451) phase 3 clinical trial (randomized, open-label, multicenter, international) is evaluating an experimental therapy in adult patients (n=1171) with previously untreated unresectable hepatocellular carcinoma at stage B (not suitable for locoregional therapy) or stage C according to the Barcelona Clinic Liver Cancer (BCLC) staging system.
Participants receive either sorafenib (400 mg twice daily) or an experimental therapy that involves either durvalumab monotherapy (1500 mg every 4 weeks) or a combination treatment of durvalumab (1500 mg every 4 weeks) with tremelimumab (one priming dose of 300 mg), called STRIDE (Single Tremelimumab Regular Interval Durvalumab).
According to an interim analysis of the data (71% maturity of these), after follow-up at a median of 32.2, 32.6, and 33.2 months, the results were as follows.
The STRIDE therapeutic regimen, which provided a median overall survival (OS) of 16.4 months (95% CI: 14.2–19.6) versus 13.8 months (95% CI: 12.3–16.1) in the sorafenib group, reduced risk of death by a relative 22%: hazard ratio (HR) 0.78 (96% 0.65–0.93; p=0.0035).
Survival at 36 months was fair for 30.7% of patients who followed the STRIDE regimen — vs. 24.7% and 20.2% of subjects in the durvalumab and sorafenib groups, respectively.
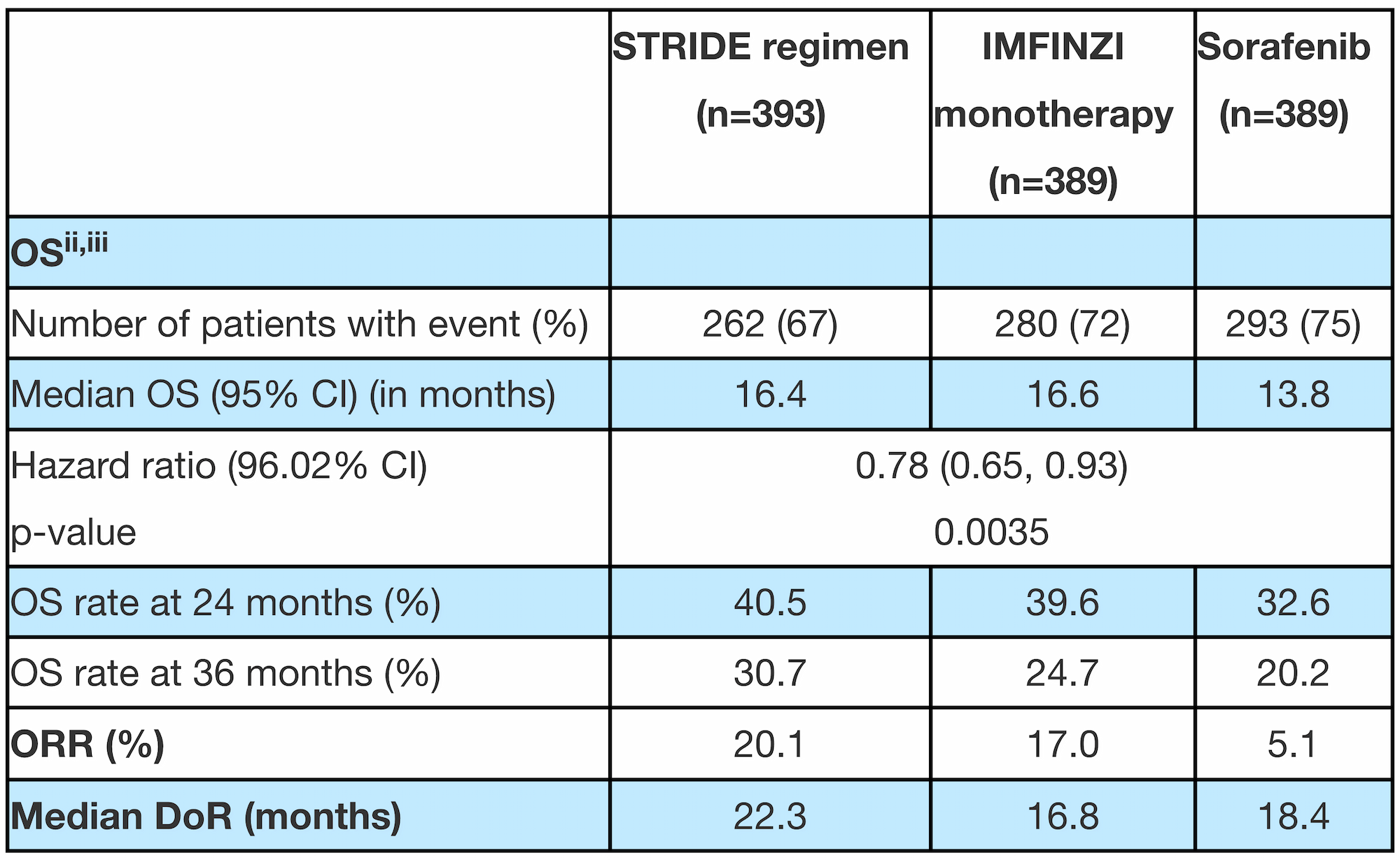
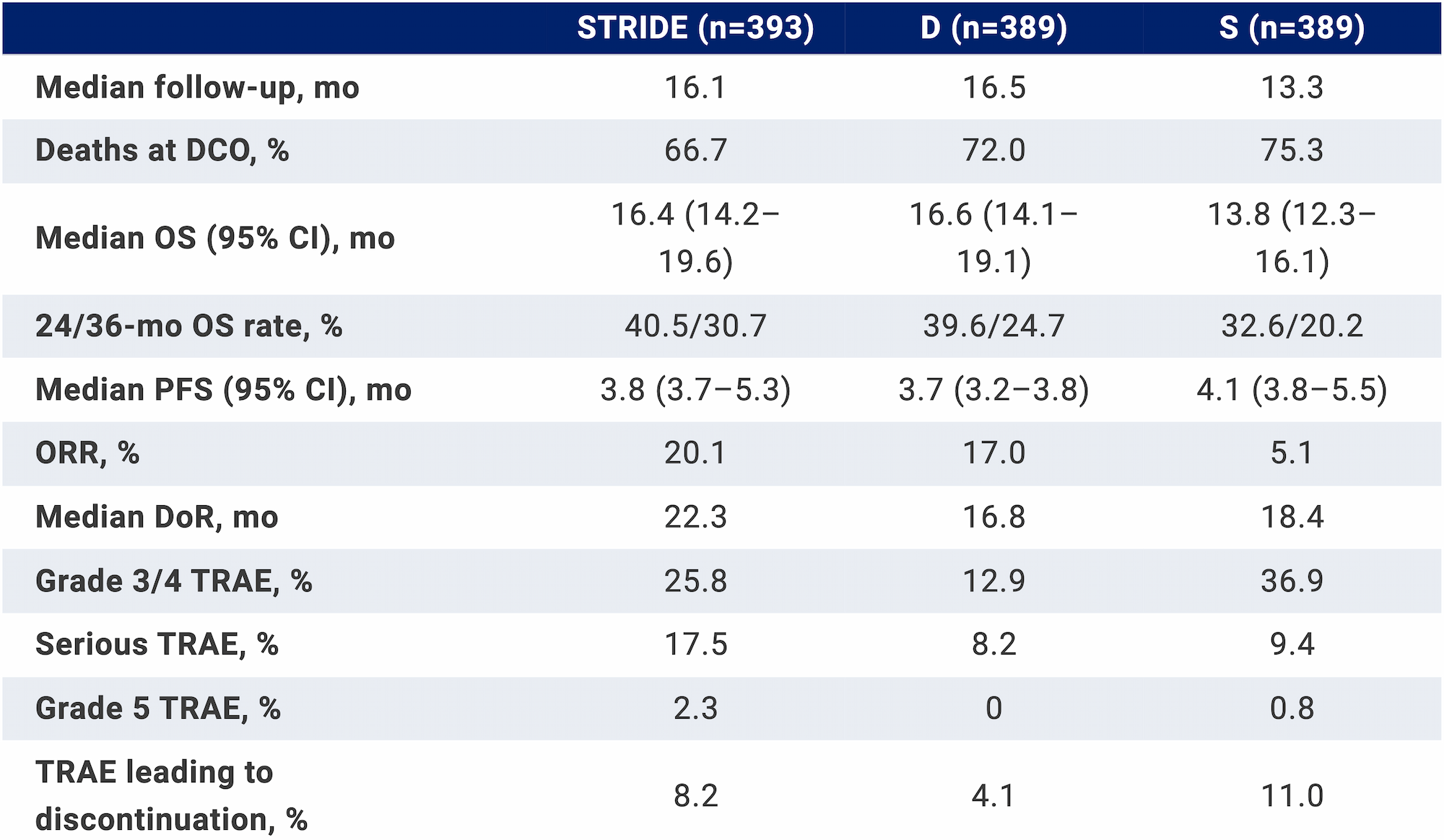
The median progression-free survival (PFS) did not differ overall between treatment groups: 3.8 (95% CI: 3.7–5.3), 3.7 (95% CI: 3.2–3.8), and 4.1 months (95% CI: 3.8–5.5). In contrast, the objective response rate (ORR), defined as at least 30% tumor regression, did so in favor of the immuno-oncology cocktail, at 20.1%, 17.0%, and 5.1%. The median duration of response (DoR) came out to 22.3, 16.8, and 18.4 months.
The safety profile of the combination of durvalumab with tremelimumab was not characterized by any new signals beyond those already known. Severe or life-threatening adverse reactions were experienced by 25.8% of patients, compared with 36.9% in the Nexavar group and 12.9% in the Imfinzi group. Adverse events forced 8.2%, 11.0%, and 4.1% of subjects to discontinue treatment, respectively.
Extras
Tecentriq (atezolizumab). Prescribing information. U.S. [PDF]
Tecentriq (atezolizumab). Prescribing information. Europe [PDF]
Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020 May 14;382(20):1894-1905. [source]
Atezolizumab + bevacizumab vs sorafenib in patients with unresectable hepatocellular carcinoma: phase 3 results from IMbrave150. HCC-TAG 2020. [PDF]
Clinical value of atezolizumab + bevacizumab for first-line unresectable hepatocellular carcinoma (HCC): a network meta-analysis. ASCO 2020. [PDF]
Time to response and characteristics of patients who had complete responses in IMbrave150: a phase III clinical trial of atezolizumab + bevacizumab vs sorafenib for unresectable hepatocellular carcinoma (HCC). ASCO 2020. [PDF]
Longitudinal and personalized detection of circulating tumor DNA (ctDNA) for monitoring treatment response with atezolizumab plus bevacizumab in patients with unresectable hepatocellular carcinoma (HCC). ASCO 2020. [PDF]
Genomic correlates of clinical benefits from atezolizumab combined with bevacizumab vs. atezolizumab alone in patients with advanced hepatocellular carcinoma (HCC). AACR 2020. [PDF]
Alpha-fetoprotein (AFP) kinetics as a potential surrogate biomarker in patients with hepatocellular carcinoma (HCC) treated with atezolizumab + bevacizumab. ILCA 2020. [PDF]
IMbrave150: management of adverse events of special interest (AESIs) for atezolizumab and bevacizumab in patients with unresectable hepatocellular carcinoma (HCC). ESMO 2020. [PDF]
IMbrave150: updated overall survival data from a global, randomized, open-label phase III study of atezolizumab + bevacizumab vs sorafenib in patients with unresectable hepatocellular carcinoma. ASCO GI 2021. [PDF]
IMbrave150: exploratory efficacy and safety results of atezolizumab + bevacizumab vs sorafenib in patients with unresectable hepatocellular carcinoma (HCC) who had prior locoregional therapy (LRT). EASL 2021. [PDF]
IMbrave150: updated efficacy and safety by risk status in patients (pts) receiving atezolizumab (atezo) + bevacizumab (bev) vs sorafenib (sor) as first-line treatment for unresectable hepatocellular carcinoma (HCC). AACR 2021. [PDF]
IMbrave150: exploratory efficacy and safety results in patients with hepatocellular carcinoma without macrovascular invasion or extrahepatic spread treated with atezolizumab + bevacizumab or sorafenib. ESMO 2021. [PDF]
Cost-effectiveness and cost-utility analyses of atezolizumab-based therapy in patients with advanced or unresectable hepatocellular carcinoma in Italy. ISPOR 2021. [PDF]
IMbrave150: exploratory efficacy and safety in patients with unresectable hepatocellular carcinoma (HCC) treated with atezolizumab beyond radiological progression until loss of clinical benefit in a global phase III study. ASCO GI 2022. [PDF]
Relationship between real-world treatment patterns and survival in patients with hepatocellular carcinoma in the US. ASCO GI 2020. [PDF]