Highlights
Japan’s StemRIM, Shionogi & Co., and Osaka University are developing the experimental drug redasemtide, the first representative of a new class of drug compounds that induce regeneration.
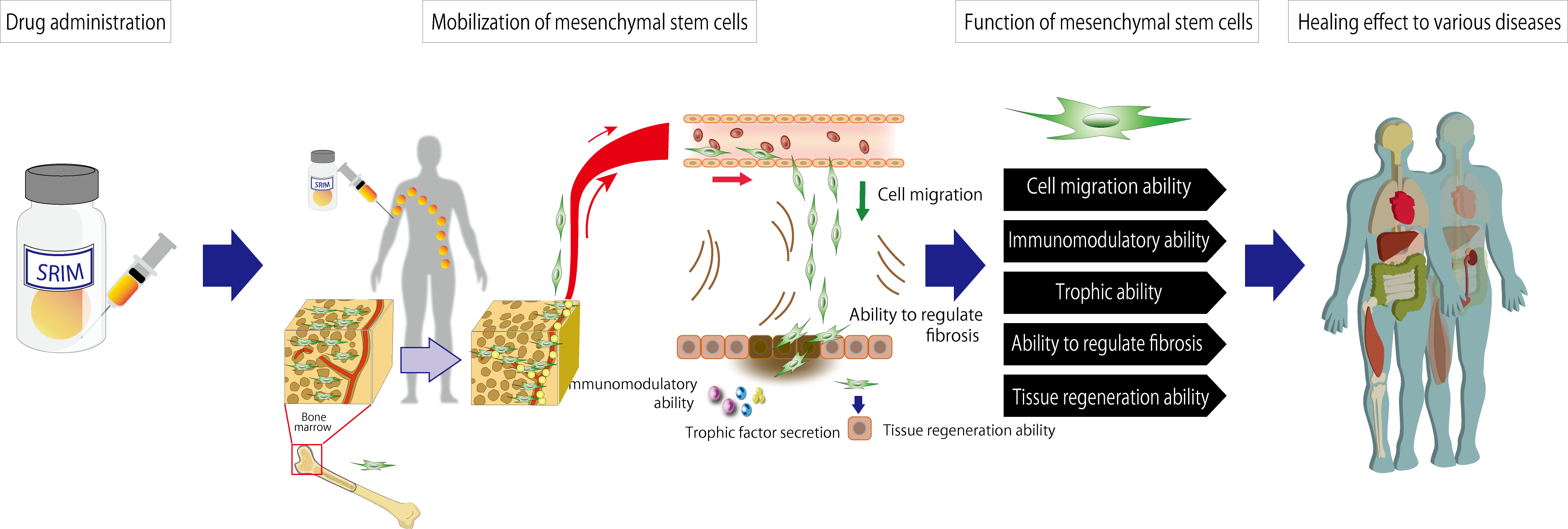
Redasemtide stimulates the functional regeneration of patient tissues and organs damaged by injury or disease by maximizing the human body’s innate ability for tissue repair. Redasemtide increases the number of circulating mesenchymal stem cells and accumulates them in damaged tissues by mobilizing bone marrow mesenchymal stem cells into the peripheral blood stream, resulting in accelerated repair of damaged tissues.
Redasemtide is a simple and relatively inexpensive pharmacological analogue of regenerative medicine (restoration of diseased or damaged tissue), complicated and expensive due to the need to produce stem cells or transplant cultured cells.
Redasemtide is undergoing extensive clinical evaluation in the treatment of diseases such as dystrophic bullous epidermolysis, cerebral infarction (acute ischemic stroke), cardiomyopathy (ischemic cardiomyopathy, dilated cardiomyopathy), osteoarthritis of the knee, chronic liver disease due to alcoholic steatohepatitis, non-alcoholic steatohepatitis (NASH), chronic hepatitis B or C.
Redasemtide: Mechanism of Action
Redasemtide (S-005151) is a stem cell modulator. After intravenous injection redasemtide triggers processes that have regenerative effects similar to those observed in regenerative medicine procedures.
Redasemtide is a peptide analogue of high mobility group box 1 (HMGB1) protein, also known as amphoterin, and includes a synthetic sequence of 44 amino acid residues belonging to the bioactive domain of HMGB1. Redasemtide does not include the functional domains of HMGB1 associated with inflammatory responses.
HMGB1 is a non-histone nuclear protein that regulates chromatin structure remodeling as a molecular chaperone in the DNA-protein chromatin complex [1].
HMGB1 performs two opposite functions: it supports tissue repair [2] and induces inflammation [3] [4] [5]
In damaged or infected tissues, HMGB1 is actively secreted by macrophages and dendritic cells or passively released from necrotic cells, thereby inducing tissue remodeling by activating inflammatory responses (i.e. macrophage and neutrophil infiltration) through binding to Toll-like receptors (TLR) and/or glycation end-product receptors on their surface [6].
In parallel, HMGB1 inhibits TLR signaling and blocks the spread of inflammation to surrounding tissues. [4] [7]
HMGB1 enhances the mobilization of bone marrow mesenchymal cells with platelet-derived growth factor receptor alpha (PDGFRα+) into the damaged tissue. [8] [9] [10]
When redasemtide is injected intravenously, mesenchymal stem (stromal) cells (MSCs) from the patient’s bone marrow are mobilized (engaged) into the peripheral blood and accumulate in the sites of injury, promoting tissue regeneration and healing of the affected areas. Due to such properties of MSCs as cell migration, immunomodulatory and trophic ability, as well as the ability to regulate fibrosis and trigger tissue regeneration, redasemtide is expected to find therapeutic application in a wide range of diseases.
Since the cells mobilized by redasemtide are ectodermal mesenchymal stem cells, a high level of their pluripotency is maintained, and since no ex vivo culturing is performed, a high level of their ability to differentiate is maintained.
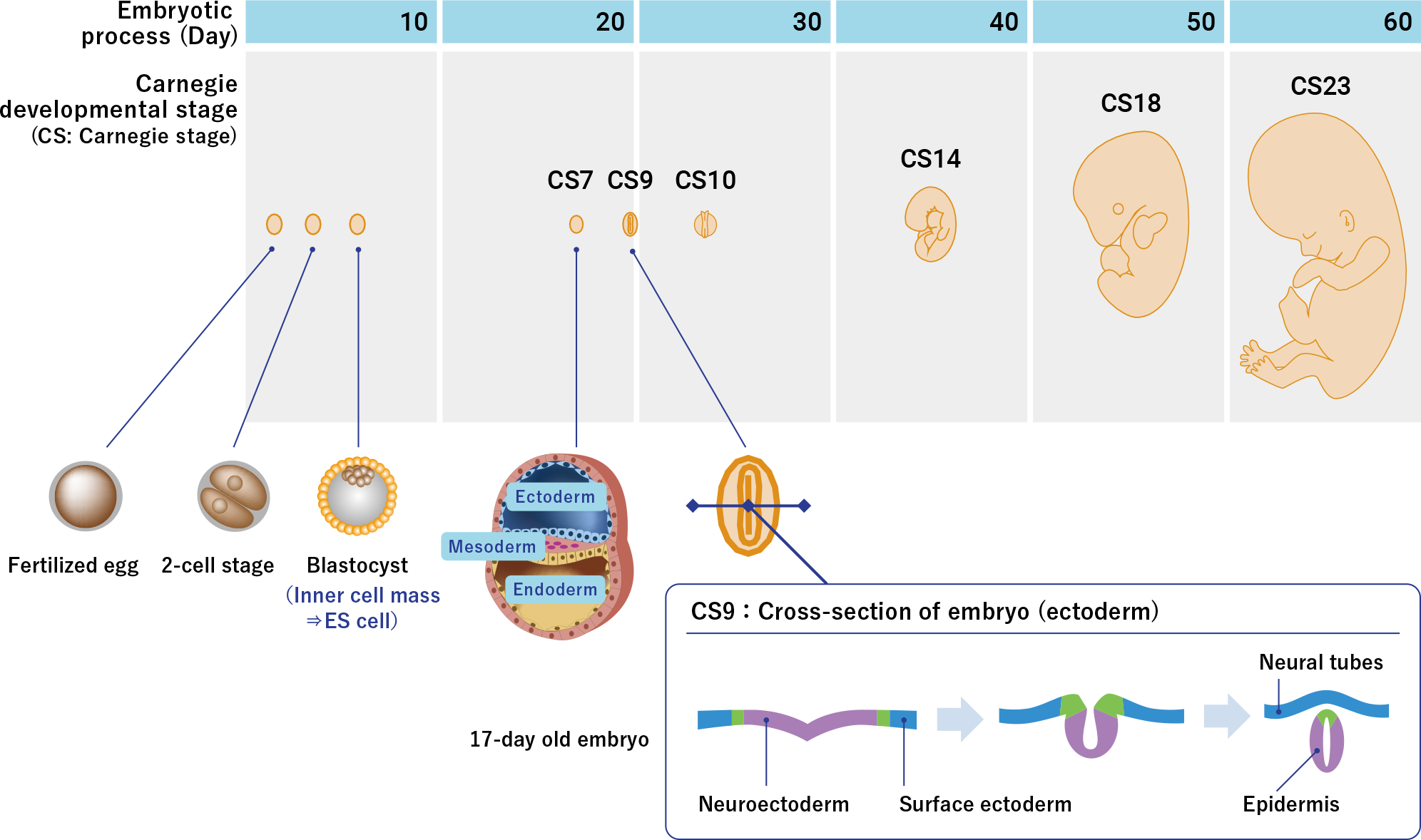
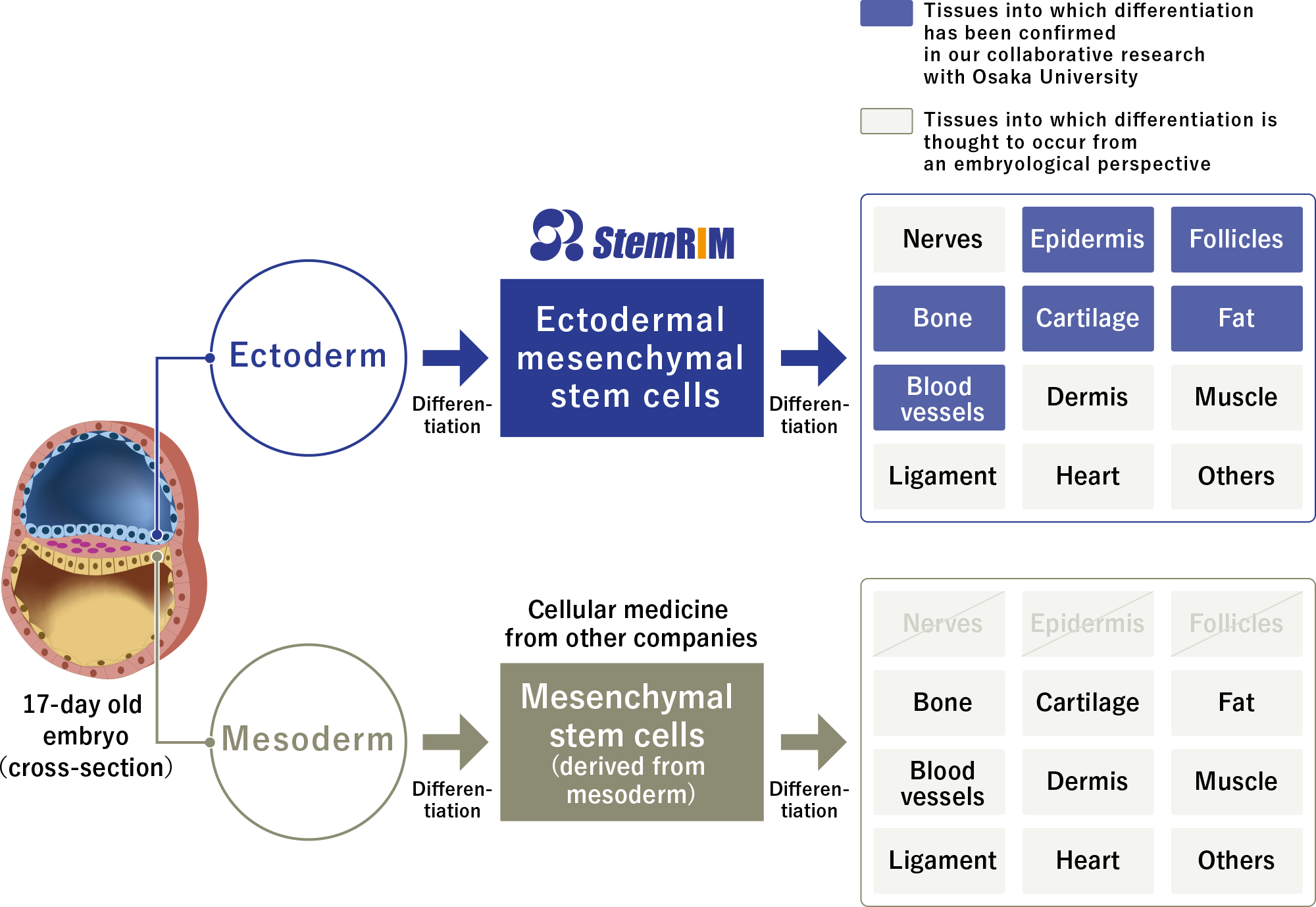
Based on the laboratory and embryological data, redasemtide is able to induce regeneration of such damaged tissues as bones (ectodermal MSCs differentiate into osteoblasts), cartilages (chondrocytes), fat (adipocytes), connective tissue (fibroblasts), skeletal muscles (myocytes), epidermal tissue (keratinocytes), nerves (neurons), and blood vessels (vascular endothelial cells).
If we talk about the practical use of redasemtide as an inducer/promoter of functional tissue regeneration, its application is seen in three directions:
- For direct treatment of diseases. Tissues damaged by various physiological conditions, injuries, burns, inflammation, autoimmune conditions, genetic disorders, etc., causing ischemia, hypoperfusion, hypoxia, necrosis. Preclinical studies in animal models confirmed the therapeutic effect of redasemtide in diseases such as cerebral infarction, myocardial infarction, cardiomyopathy, bullous epidermolysis, hard-to-treat skin ulcers, spinal cord injury, amyotrophic lateral sclerosis, traumatic brain injury, ulcerative colitis.
- For indirect treatment of diseases. Redasemtide can be an alternative to invasive harvesting of MSCs from the bone marrow. A method of subcutaneous implantation of a medical device with redasemtide, which collects the MSCs from peripheral blood, has been proposed; the obtained cells are subsequently transplanted into the area of tissue damage.

- For diseases prevention. Redasemtide can be used as a prophylactic drug that prevents tissue dysfunction or deterioration of tissue functions caused by a decrease in the number of tissue stem cells, or as an anti-aging drug that slows the progression of age-related changes.
StemRIM, which emerged from the walls of Osaka University in 2006, is behind the discovery and development of redasemtide.
Redasemtide: Clinical Evaluation
Dystrophic Epidermolysis Bullosa
The UMIN000029962 phase 2 (non-randomized, open-label) clinical trial invited patients (n=9) with dystrophic epidermolysis bullosa (DEB).
Participants received intravenous redasemtide 1 mg/kg: once a day for four consecutive days in the first week, twice a week from week 2 to week 4, for a total of 10 infusions.
The primary efficacy endpoint of treatment was determined by the rate of change in the total area of blisters, erosions, and ulcers throughout the body compared with baseline.
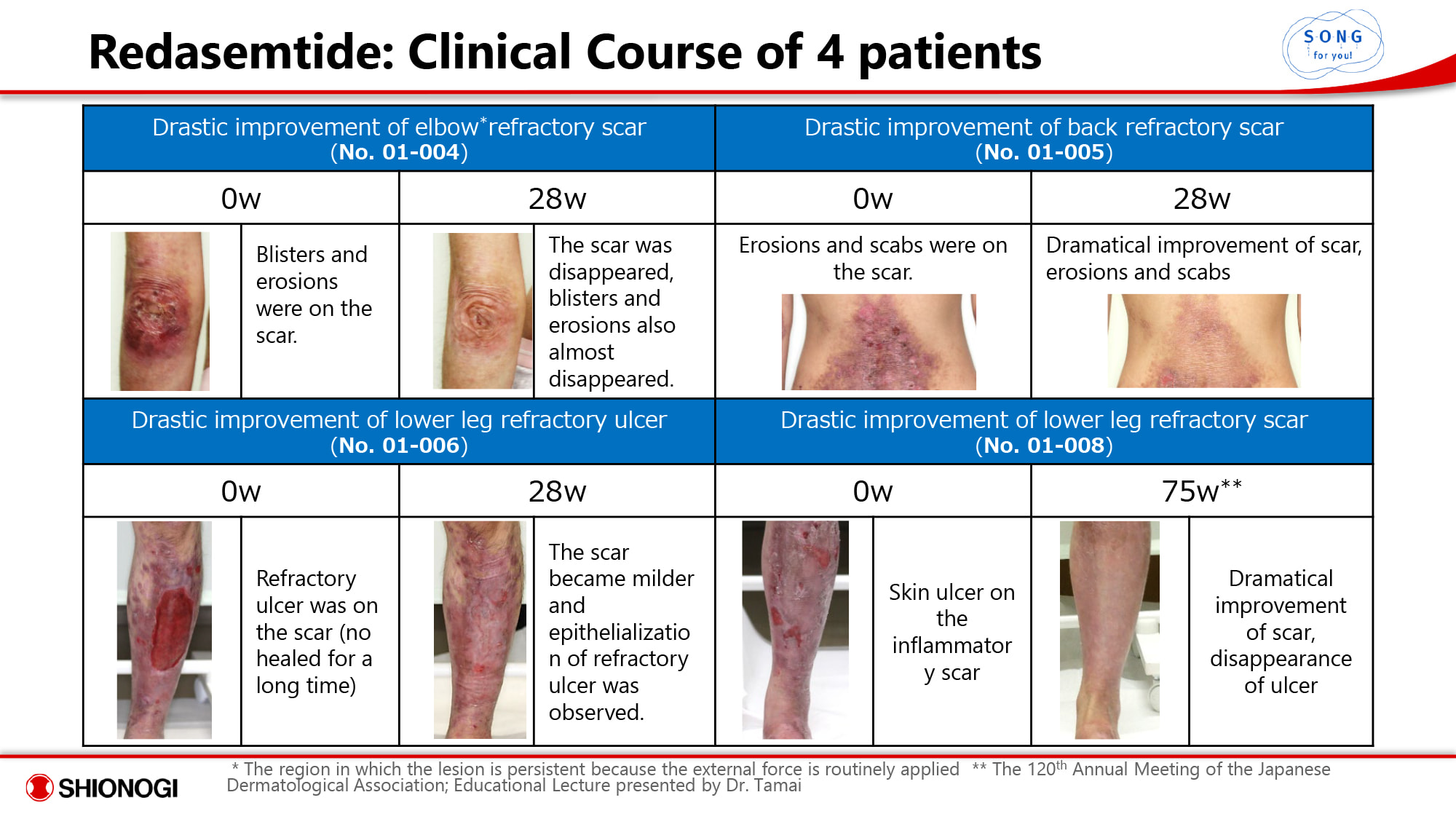
At the end of the 28-week follow-up (followed up in the JapicCTI-194798 observational clinical trial), 78% of subjects (n=7/9) showed statistically significant improvement, with 44% (n=4/9) recording a complete response with lesion area as close to zero as possible. Patients reported disappearance, softening, or improvement of scars, blisters, erosions, scabs, and epithelialization of refractory ulcers.

Despite redasemtide’s successful clinical trial in the treatment of dystrophic epidermolysis bullosa, another efficacy-confirming clinical study is needed before the application can be submitted to the regulator. This is likely to take a long time, since there are decidedly not enough patients with the disease.
Currently, there is no approved treatment for dystrophic epidermolysis bullosa, therapy is limited to palliative care. In the near future, Krystal Biotech will try to offer a gene therapy topical Vyjuvek (beremagene geperpavec), which has been very successful in treating this rare and severe genetic disease.

Vyjuvek: Effective Treatment for Dystrophic Epidermolysis Bullosa
Krystal Biotech’s beremagene geperpavec gene therapy will save from imminent death.
Acute Ischemic Stroke
The JapicCTI-194963 phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled elderly (60–80 years old) patients (n=150) with acute ischemic stroke who were not suitable for revascularization therapy, including thrombolytic therapy (infusion of tissue plasminogen activators) and mechanical thrombectomy (intravascular recanalization).
Among the main inclusion criteria: supratentorial ischemic stroke confirmed by MRI; no more than 4.5–24 hours after ischemic stroke manifestation; the National Institutes of Health Stroke Scale (NIHSS) stroke severity score of 8–22; no rapid change in neurological signs within 30 minutes before enrollment.
Subjects received intravenous placebo or redasemtide 1.5 mg/kg once daily for 5 days.
The primary efficacy endpoint of the treatment was the modified Rankin Scale (mRS) score, which assesses the degree of disability after 90 days of treatment.
In mid-December 2021, Shionogi & Co. announced the success of a clinical trial of redasemtide in the treatment of acute ischemic stroke, thereby giving hope for a radically new treatment for this very common pathological condition that is now successfully managed within a very narrow therapeutic window. The results will be published later. A phase 3 clinical trial is being prepared for launch.
Knee Osteoarthritis
The jRCT2021200034 phase 2 (randomized, double-blind, placebo-controlled) clinical trial of redasemtide in adult patients (n=20) with medial knee osteoarthritis who underwent high tibial osteotomy and arthroscopic microfracture continues.
Immediately after surgery, participants receive intravenous placebo or redasemtide 1.5 mg/kg, for a total of 8 infusions every 3–4 days for 4 weeks.
Then, after 48 weeks, the efficacy of redasemtide relative to placebo in terms of morphological and functional changes in the knee joint is evaluated, including histological and MRI assessments, the Kellgren–Lawrence radiological severity scale, the Knee Injury and Osteoarthritis Outcome Score (KOOS), the Lysholm knee scoring scale, the Western Ontario and McMaster University Osteoarthritis Index (WOMAC) assessments.
Chronic Liver Disease
The jRCT2031200232 phase 2 (non-randomized, open-label) clinical trial of redasemtide among adult patients (n=10) with chronic liver disease is ongoing.
Participants must have the following condition: alcoholic steatohepatitis (alcohol abstinence for more than 6 months), non-alcoholic steatohepatitis (NASH) [on physical and dietary therapy for more than 6 months], chronic hepatitis B (negative for viral DNA for at least 6 months after antiviral therapy), chronic hepatitis C (sustained virologic response for more than 12 months after antiviral treatment).
Among the main inclusion criteria: severity of liver cirrhosis of 7 points or less according to the Child–Pugh score; liver stiffness measured by magnetic resonance elastography (MRE) greater than 4 kPa; pathophysiology must be characterized by stability in the 3-month follow-up period preceding the start of the study.
Participants receive intravenous redasemtide 1.5 mg/kg in two different regimens: either 4 infusions weekly or 7 infusions (first 4 weekly, then on days 8, 15, and 22).
The efficacy of treatment is analyzed during 28 weeks of observation by evaluating fibrosis and inflammation of the liver and its functional characteristics.
Cardiomyopathy
Preparations are underway to launch a phase 2 clinical trial that will test the suitability of redasemtide in the treatment of ischemic cardiomyopathy or dilated cardiomyopathy.
Tissue Regeneration: What’s Next
The scientific expertise of StemRIM, which extends beyond just one redasemtide, suggests further development of drugs that provide regeneration of damaged tissues.
Thus, the experimental peptide drug RIM3, which mobilizes bone marrow mesenchymal stem cells, is undergoing preclinical testing in the therapy of ulcerative colitis and atopic dermatitis (eczema).
The StemRIM experimental pipeline contains protein drugs (derived from body proteins extracted from living tissue), which, when administered intravenously or topically, attract and accumulate mesenchymal stem cells in a different way than redasemtide and its analogues. For example, if the area of tissue damage is small (or the damage is not in the acute phase), the level of stromal cell-derived factor 1 (SDF-1, CXCL12), as one of the triggers of cell mobilization under hypoxia, is low, and therefore MSCs are not attracted and accumulate in the proper amount. In such a situation, injection of the developed protein drug, an analogue of SDF-1, into the periphery of the lesion to accumulate MSCs in the circulatory system close to the treated organ can help.

StemRIM also proposed the idea of gene therapy based on mesenchymal stem cells. In the case of a genetic disease, the required functional gene is transfected ex vivo into MSCs collected from the patient by apheresis, which are then returned back into the body. In addition to the proper therapeutic effect, we can expect both the absence of immune rejection reactions and long-term action due to the immune tolerance of such cells.
Extras
Shionogi R&D Day 2021. September 29, 2021. [PDF]
StemRIM. Non-consolidated financial results for the fiscal year ended July 31, 2021. September 9, 2021. [PDF]
Agent for recruitment of bone-marrow-derived pluripotent stem cell into peripheral circulation. WO2009133939A1. [source]
Synthesized HMGB1 peptide attenuates liver inflammation and suppresses fibrosis in mice. Inflamm Regen. 2021 Sep 27;41(1):28. [source]
High-mobility group box 1 fragment suppresses adverse post-infarction remodeling by recruiting PDGFRα-positive bone marrow cells. PLoS One. 2020 Apr 10;15(4):e0230392. [source]
The administration of high-mobility group box 1 fragment prevents deterioration of cardiac performance by enhancement of bone marrow mesenchymal stem cell homing in the delta-sarcoglycan-deficient hamster. PLoS One. 2018 Dec 5;13(12):e0202838. [source]
Stem cell therapy for epidermolysis bullosa—does it work? J Invest Dermatol. 2016 Nov;136(11):2119-2121. [source]
Endogenous mesenchymal stromal cells in bone marrow are required to preserve muscle function in mdx mice. Stem Cells. 2015 Mar;33(3):962-75. [source]
Transplanted bone marrow-derived circulating PDGFRα+ cells restore type VII collagen in recessive dystrophic epidermolysis bullosa mouse skin graft. J Immunol. 2015 Feb 15;194(4):1996-2003. [source]
Systemic high-mobility group box 1 administration suppresses skin inflammation by inducing an accumulation of PDGFRα(+) mesenchymal cells from bone marrow. Sci Rep. 2015 Jun 5;5:11008. [source]
PDGFRalpha-positive cells in bone marrow are mobilized by high mobility group box 1 (HMGB1) to regenerate injured epithelia. Proc Natl Acad Sci U S A. 2011 Apr 19;108(16):6609-14. [source]