Highlights
Empaveli (pegcetacoplan) is a new drug indicated for treating paroxysmal nocturnal hemoglobinuria in adults.
Empaveli, developed by Apellis Pharmaceuticals, is approved by the U.S. Food and Drug Administration (FDA) in May 2021.
The European Medicines Agency (EMA) issued marketing authorization for Aspaveli (pegcetacoplan) in mid-December 2021. Aspaveli is indicated in the treatment of adult patients with paroxysmal nocturnal haemoglobinuria who are anaemic after treatment with a C5 inhibitor for at least 3 months.
Empaveli is ahead of Alexion Pharmaceuticals’ Soliris (eculizumab), which, except for its more patient-friendly Ultomiris (ravulizumab) variant, is the only approved drug to treat paroxysmal nocturnal hemoglobinuria.
First, pegcetacoplan provided a decent increase in hemoglobin. Second, pegcetacoplan eliminated the need for red blood cell transfusions in the vast majority of patients. Third, its use resulted in normalization of hematological markers reflecting the presence of hemolysis and a clear relief of symptoms of fatigue. And all this regardless of the severity of the course of paroxysmal nocturnal hemoglobinuria, according to the frequency of hemotransfusion procedures.
Empaveli has an obvious destiny to become the new standard of therapy for paroxysmal nocturnal hemoglobinuria. Yes, Soliris and Ultomiris generally help patients but many patients still both suffer from severe anemia and marked fatigue and require frequent blood transfusions. And all this on the background of prescribing higher than recommended doses of eculizumab.

Empaveli: Clinical Efficacy of Pegcetacoplan in Treatment of Paroxysmal Nocturnal Hemoglobinuria
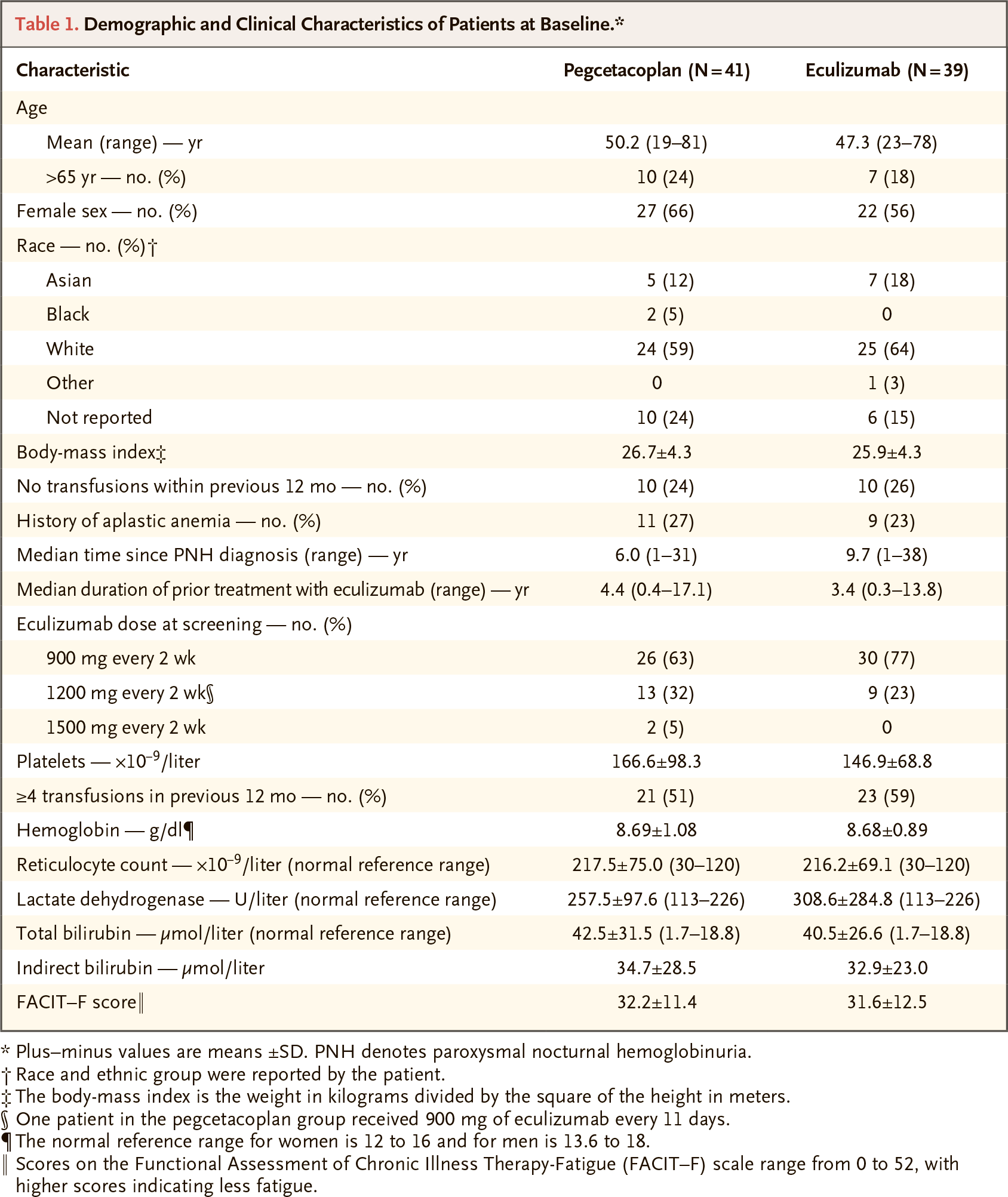
The PEGASUS (NCT03500549) phase 3 (randomized, open-label, active-controlled, multicenter, international) clinical trial enrolled adult patients (n=80) with paroxysmal nocturnal hemoglobinuria and hemoglobin levels < 10.5 g/dL, despite following a course of stable Soliris therapy.
Among the main requirements for inclusion in the study:
- absolute reticulocyte count > upper limit of normal
- platelet count > 50×109/L
- absolute neutrophil count > 0.5×109/L.
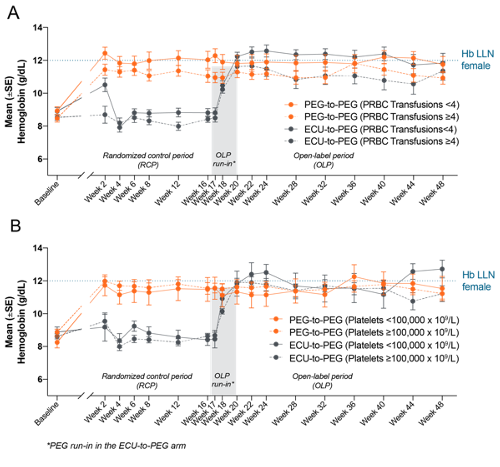
Subjects first underwent a 4-week run-in phase; all received pegcetacoplan on eculizumab. Patients were then randomized; one group followed the pegcetacoplan course (subcutaneous infusions of 1080 mg twice weekly or once every three days), while the other group continued with the familiar intravenous Soliris.
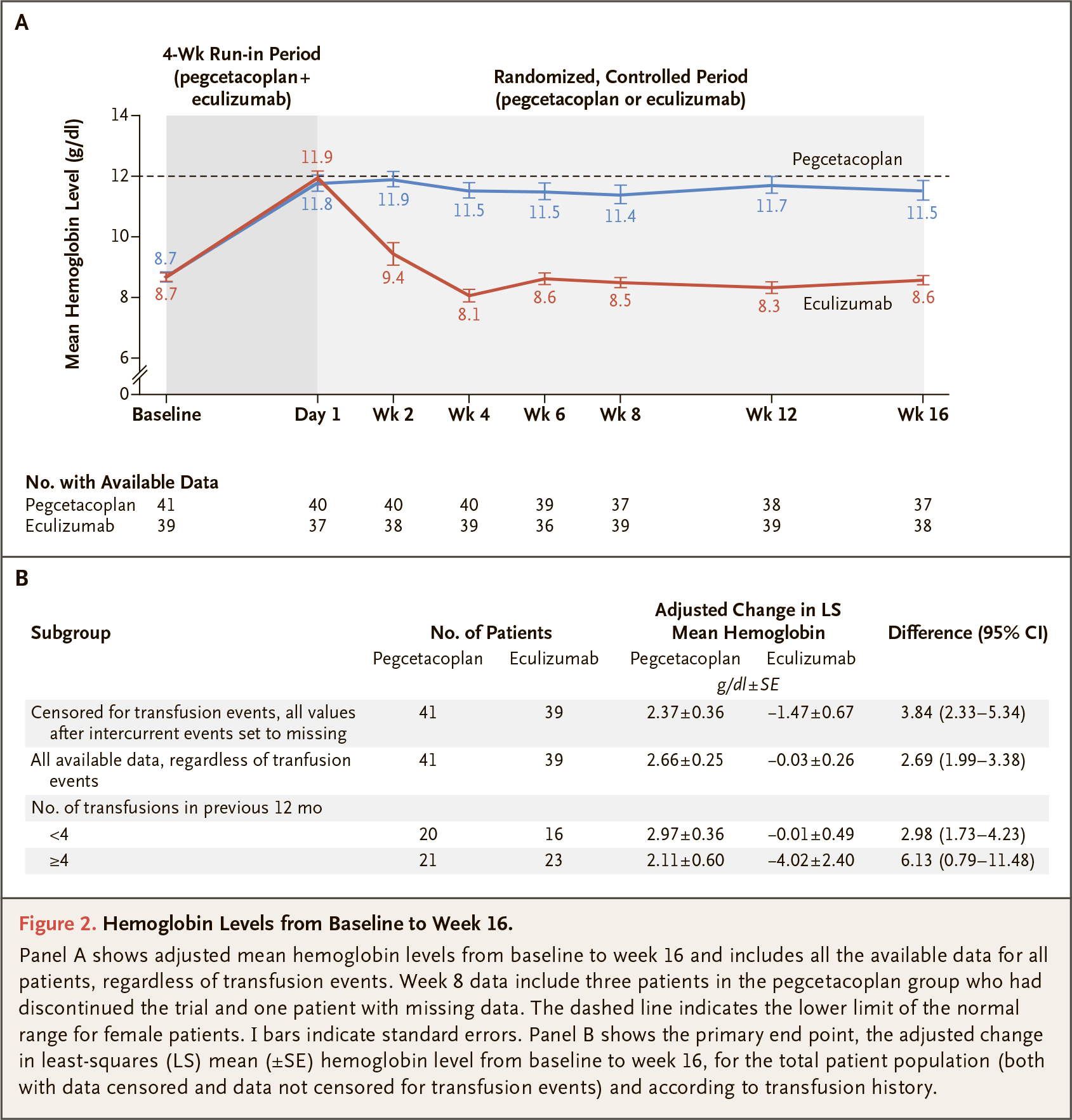
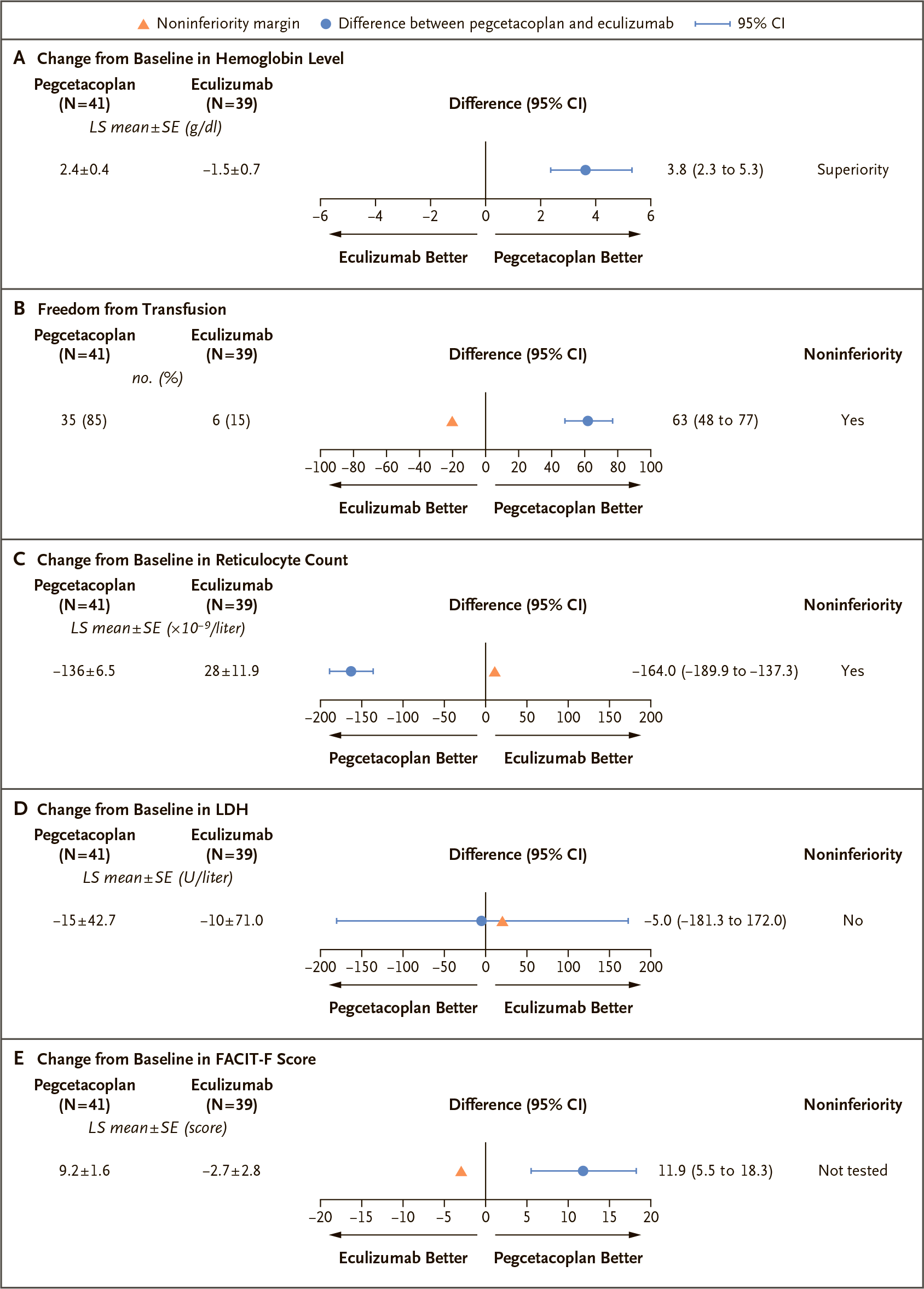
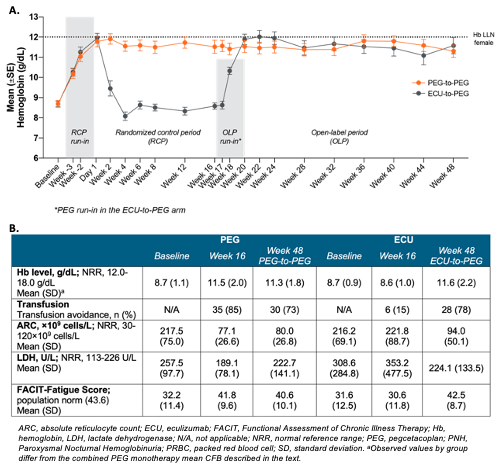
After 16 weeks, the primary endpoint determined by the change in hemoglobin levels was assessed. Patients receiving pegcetacoplan showed a statistically significant advantage over the eculizumab group; their hemoglobin rose by an average of 2.37 g/dL versus a decrease of 1.47 g/dL. The final adjusted mean difference was 3.84 g/dL (95% CI: 2.33–5.34); p<0.0001. In other words, Empaveli provided a 53% increase in hemoglobin levels compared to Soliris.
Hemoglobin levels, which began to rise after two weeks of treatment with pegcetacoplan, were within normal limits in 34% of participants, compared to 0% in the Soliris group.
The subgroup of patients not requiring transfusions or only slightly dependent on them (less than 4 transfusions in the last 12 months) showed a hemoglobin increase of 2.97 g/dL versus a decrease of 0.01 g/dL in the control group — from the initial 8.9 g/dL.
Among patients who were highly dependent on transfusions (4 or more transfusions in the last 12 months), pegcetacoplan was even more effective compared to eculizumab; the hemoglobin increase was 2.11 g/dL versus a decrease of 4.02 g/dL — from the initial 8.5 g/dL.
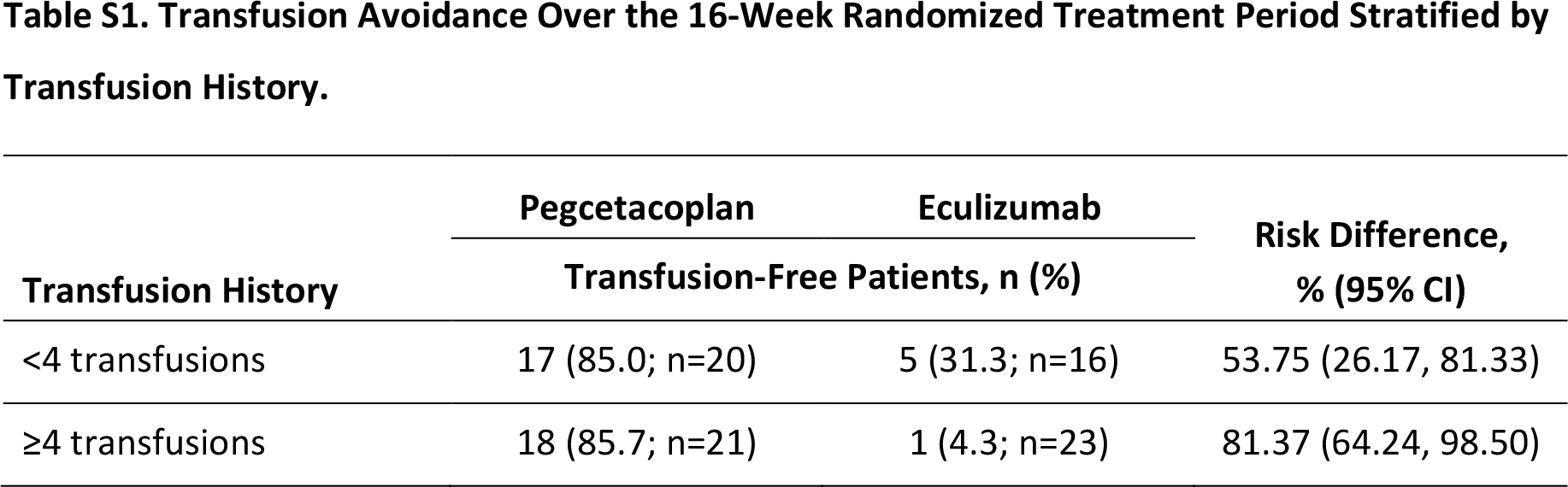
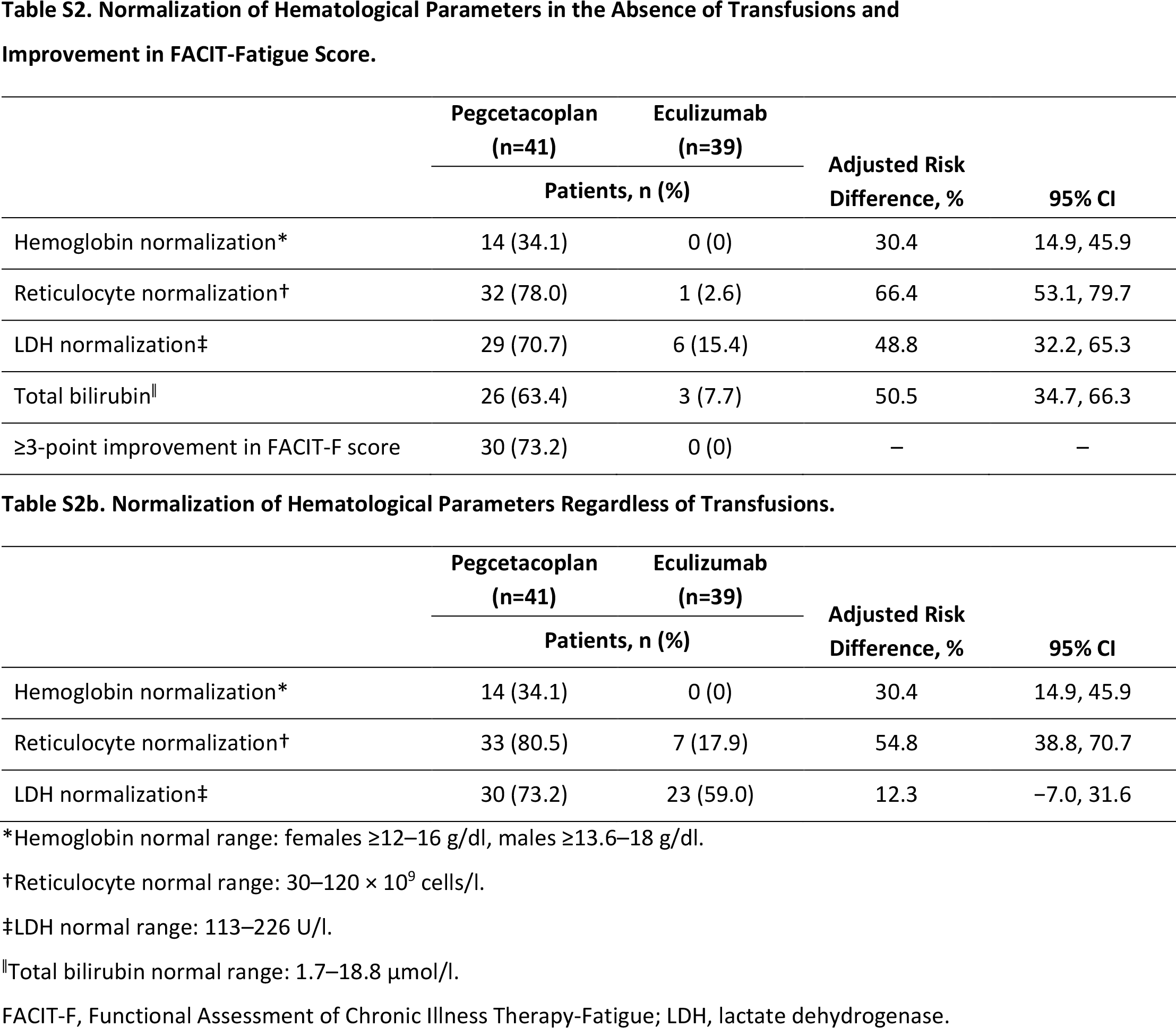
The treatment of paroxysmal nocturnal hemoglobinuria with pegcetacoplan resulted in 85% of patients not requiring blood transfusions at all during the 16-week therapy period: 85% and 86% of patients in the low and high hemotransfusion-dependent subgroups. In contrast, only 15% of subjects did not resort to such a procedure when prescribed Soliris: 31% and 4%, respectively.
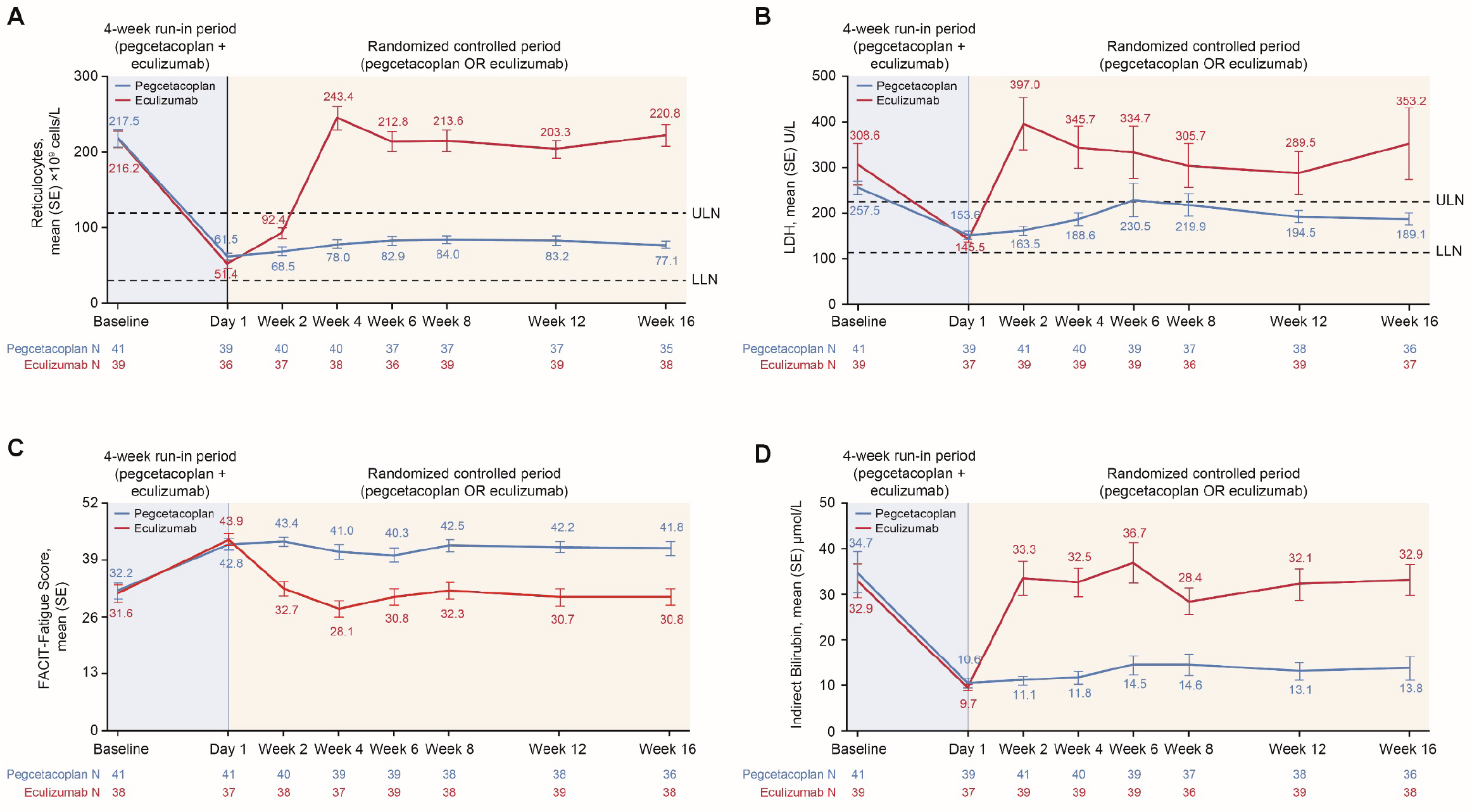
Pegcetacoplan endowed patients with stabilization of hematological markers reflecting the degree of hemolysis. Thus, normalization of absolute reticulocyte count and lactate dehydrogenase (LDH) levels, which indicate extravascular and intravascular hemolysis, respectively, was fair for 81% and 73% of subjects without reference to hemotransfusion need status — versus 18% and 59%, respectively. However, a statistically significant difference between Empaveli and Soliris was recorded only with respect to the normalization of reticulocyte count.
Pegcetacoplan relieved symptoms of fatigue, experienced by almost all patients with paroxysmal nocturnal hemoglobinuria, which decisively impairs quality of life: a change of at least 3 points (clinically significant) in the fatigue score on the FACIT-F (Functional Assessment of Chronic Illness Therapy–Fatigue) scale was documented for 73% of respondents — versus 0% for the Soliris group. Overall, Empaveli increased FACIT-F by 9.2 points versus a 2.7 point decrease in the Soliris group, a difference of 11.9 points (95% CI: 5.49–18.25).
Additional data collected during an additional 32 weeks of pegcetacoplan therapy as part of PEGASUS confirmed its long-term efficacy in terms of normalizing hemoglobin and the abovementioned hematological parameters. Remarkably, the effectiveness of pegcetacoplan therapy did not depend on either the baseline platelet count or the initial severity of the disease. At 48 weeks of treatment, 73% of patients did not require transfusions.
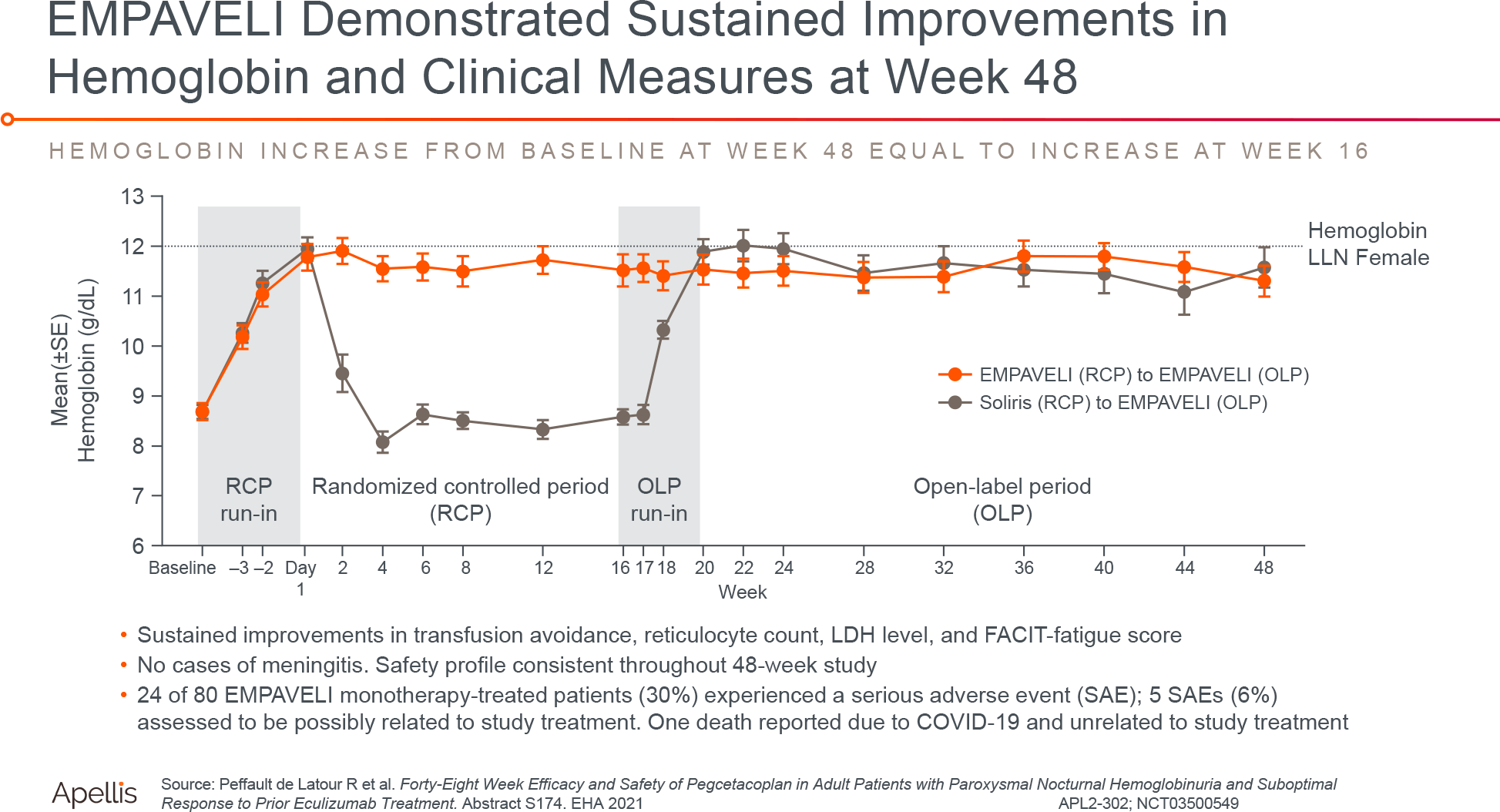
A 48-week treatment of paroxysmal nocturnal hemoglobinuria with pegcetacoplan resulted in 63% of patients reaching good, major, or complete hematologic response status. A good hematologic response was defined as no need for transfusions but with chronic mild anemia or evidence of hemolysis; a major hematologic response was defined as no need for transfusions and normal hemoglobin levels but with evidence of hemolysis; a complete hematologic response was defined as no need for transfusions, stabilized hemoglobin levels and no evidence of hemolysis.

Empaveli: Safety of Pegcetacoplan in Treatment of Paroxysmal Nocturnal Hemoglobinuria
The prescribing information for Empaveli has a black-box warning regarding the risk of infections caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis types A, C, W, Y, and B, Haemophilus influenzae type B. The course of infections can be serious, life-threatening, or even fatal. And therefore, all patients treated with Empaveli, which suppresses the immune system, must necessarily be vaccinated against these pathogens in advance.
The adverse reactions to treatment experienced by 88% and 87% of patients in the pegcetacoplan and eculizumab groups, respectively, were mostly mild in severity.
Among the pegcetacoplan-specific adverse events: injection site reactions, which were mild and occurred early in the clinical trial (in 37% of patients versus 7% in the eculizumab group) and mild diarrhea (22% versus 3%). Specific adverse reactions to eculizumab included headache (in 23% of patients versus 7% in the pegcetacoplan group) and fatigue (15% versus 5%).
The occurrence of infections was noted in 29% of subjects treated with Empaveli — versus 26% of patients treated with Soliris. No cases of meningitis were reported.
Events of breakthrough hemolysis were noted for 10% of patients in the pegcetacoplan group and 23% in the eculizumab group. In the case of pegcetacoplan, all such patients had LDH levels more than 3 times the upper limit of normal. Breakthrough hemolysis was said to be associated with a rapid rise in LDH levels indicative of intravascular hemolysis and occurred without identifiable triggers or detectable antibodies against pegcetacoplan.

Without the consideration of the impressive efficacy of pegcetacoplan, a long-term balance between risks and benefits must be ensured, because excessive complement suppression on chronic paroxysmal nocturnal hemoglobinuria therapy leaves the body without the first line of defense from the innate immune system. That’s why Apellis collected data from subjects in PEGASUS who agreed to continue participation in this clinical trial for an additional 32 weeks.
At 48 weeks of Empaveli use, the most common adverse events were injection site reactions (in 36% of patients), hemolysis (24%), and diarrhea (21%). However, 30% of patients experienced serious adverse reactions, of which 6% are thought to be related to pegcetacoplan therapy. No cases of meningitis were noted.
Empaveli: Mechanism of Action of Pegcetacoplan
Pegcetacoplan (APL-2) is a synthetic cyclic peptide conjugated to polyethylene glycol and binds to complement system component 3 (C3) and its C3b fragment. The molecule is a derivative of compstatin (compstatin), a cyclic peptide, created at the University of Pennsylvania, which irreversibly binds to C3 and its fragments C3b and C3c.
C3 inhibition is thought to block all pathways of complement activation — classical, lectin, and alternative. Additionally, it is blocking C3 that suppresses all three principal immune responses — opsonization, inflammation, and membrane attack complex (MAC) formation.
Eculizumab and ravulizumab work differently. These humanized monoclonal antibodies bind to complement system component 5 (C5) and inhibit its cleavage into C5a and C5b terminal fragments which prevents the formation of the complement terminal complex C5b-9 which in turn gives rise to MAC.
Pegcetacoplan: What’s Next
In the second quarter of 2021, results will be available from the PRINCE (NCT04085601) phase III clinical trial testing pegcetacoplan in patients who have not previously been treated for paroxysmal nocturnal hemoglobinuria. The need for this trial was because Apellis did not know what the regulator’s verdict would be; there were concerns that the FDA would only allow pegcetacoplan for those who were already being treated with Soliris, and it was not particularly helpful.
In parallel, Apellis is conducting an extensive clinical evaluation of the applicability of pegcetacoplan in the therapy of other diseases mediated (proven or suspected) by the complement such as:
- geographic atrophy (GA) secondary to age-related macular degeneration (AMD)
- intermediate AMD
- autoimmune hemolytic anemia (AIHA): warm autoimmune hemolytic anemia (WAIHA) and cold agglutinin disease (CAD)
- hematopoietic stem cell transplant-associated thrombotic microangiopathy (HSCT-TMA)
- nephropathy: IgA nephropathy (IgAN), lupus nephritis (LN), primary membranous nephropathy (PMN), and C3 glomerulopathy (C3G) including C3 glomerulonephritis (C3GN), dense deposit disease (DDD), and membranoproliferative glomerulonephritis (MPGN)
- sporadic amyotrophic lateral sclerosis (ALS).
The intravenous formulation of pegcetacoplan is seen as interesting and is being studied in the task of preventing the body’s immune attack on adenoviral vectors by which the gene therapy drugs are delivered.
The high interest in pegcetacoplan is understandable because one can make a pretty decent profit on this drug. Since its commercial debut in May 2007, Soliris, as one of the most expensive drugs on the planet, has pocketed over $30 billion.
By the way, Apellis will share pegcetacoplan revenues with Sweden’s Sobi (Swedish Orphan Biovitrum), which has acquired commercial rights outside the United States for the drug’s systemic formulation. In return, Apellis received $250 million upfront and future payments of $995 million, plus double-digit royalties on sales.
Empaveli: Prospects for Pegcetacoplan
Currently, the only complaint about Empaveli is the way and regimen of its administration: the drug is administered twice a week as subcutaneous infusions with a pump. Infusions of pegcetacoplan are conducted within 60 minutes or 30 minutes (if infusions are performed in two sites simultaneously. The infusions, however, are self-administered by the patient.
In comparison, Soliris and Ultolmiris in maintenance therapy require healthcare staff-performed intravenous infusions of 40 minutes every two or eight weeks, respectively. However, Alexion is working on a subcutaneous version of Ultolmiris administered by the patient once a week.
Be that as it may, the arrival of Empaveli is a serious blow to the business of AstraZeneca which bought Alexion for $39 billion.

AstraZeneca + Alexion = Rescue of Both Companies
Alexion Pharmaceuticals, which owns Soliris, one of the most expensive drugs on Earth, has agreed to sell AstraZeneca for $39 billion.
The appearance of eculizumab biosimilars is not far off so Alexion is methodically transferring patients from Soliris to Ultomiris. It is stated that ravulizumab therapy already covers 70% of patients previously treated with eculizumab; we are talking about American, German, and Japanese patients, they bring two-thirds of revenues. The efficacy of Soliris or Ultomiris therapy for paroxysmal nocturnal hemoglobinuria is generally identical.
Apellis is aware that, first, it is difficult to break the resistance of the medical community, which is used to the pharmacological hegemony of Alexion, and, second, it is necessary to convince health systems and insurance services of the superiority of Empaveli. And so, all involved parties should be provided with as much evidence as possible about the benefits of pegcetacoplan.
For example, pegcetacoplan outperformed ravulizumab on the following criteria after 26 weeks of treatment, according to a matching-adjusted indirect comparison (MAIC) methodology:
- FACIT-F (more is better): the mean increase in the pegcetacoplan group was 10.47 (95% CI: 6.98–13.95), which statistically significantly (p<0.001) outperformed the increase of 2.01 points (95% CI: 0.64–3.38) in the ravulizumab group
- European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-30) [pegcetacoplan demonstrated clinically significant improvements in the domains below]:
- global health status (more is better): +16.59 (95% CI: 10.34–22.84) — versus +1.15 (95% CI: −2.14 – +4.44) [p<0.001]
- physical functioning (more is better): +15.58 (95% CI: 10.53–20.62) — vs. +3.26 (95% CI: 1.53–4.99) [p<0.001]
- fatigue symptoms (less is better): −21.34 (95% CI: −30.96 — −11.72) — vs. −4.97 (95% CI: −8.40 — −1.54) [p<0.010].
Apellis claims its Empaveli is more effective than Ultomiris at stabilizing hemoglobin (76% more patients achieve this), eliminating transfusion dependence (71% more patients), normalizing LDH (64% more patients), and relieving symptoms of fatigue (3 times stronger).

In the U.S., the wholesale acquisition cost (WAC) for Empaveli is billed at $458,000 per year. That’s as much as Alexion is asking for Ultomiris but less than the $678,000 Soliris costs. Industry experts assumed that Apellis would not be greedily putting the price tag on pegcetacoplan in the range of $300,000 per year.
Nevertheless, Apellis’ stock quotes added 20%.
Extras
Empaveli (pegcetacoplan). Prescribing information. U.S. [PDF]
Empaveli (pegcetacoplan). Prescribing information. Europe. [PDF]
Pegcetacoplan versus eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2021 Mar 18;384(11):1028-1037. [source]
Empaveli (pegcetacoplan). FDA approval conference call. Apellis Pharmaceuticals. May 17, 2021. [PDF]
Targeted C3 therapies. J.P. Morgan Healthcare Conference. Apellis Pharmaceuticals. January 12, 2021. [PDF]
Pegcetacoplan. PEGASUS phase 3 positive top-line results conference call. Apellis Pharmaceuticals. January 7, 2020. [PDF]