Bemarituzumab is a promising monoclonal antibody for the first-line treatment of inoperable FGFR2b-positive HER2-negative gastric or gastroesophageal junction cancer.
In November 2020, Five Prime Therapeutics, the company behind the development of bemarituzumab, reported the success of a clinical trial of this drug candidate: treatment efficacy surpassed the standard chemotherapy approach. On the back of the news, Five Prime’s stock price jumped 400%.
If bemarituzumab is confirmed in a pivotal clinical trial, we will have the first new targeted treatment for gastric cancer in more than a decade.
To put the optimistic future in perspective: first, FGFR2b-positive gastric cancer accounts for one-third of all its diagnoses; second, HER2-positive gastric cancer accounts for no more than 10–20% of its cases. In other words, bemarituzumab will prove suitable for treating a very large patient population.
There are also strong indications that bemarituzumab will also work effectively in other FGFR2b-expressing cancers.
In early March 2021, Amgen announced the acquisition of Five Prime Therapeutics. The deal, expected to close by the end of the second quarter, is approximately $1.9 billion in cash: at $38 per Five Prime’s share (78% premium).
There are other candidate drugs on Five Prime’s pipeline that are said to seamlessly complement Amgen’s oncology expertise.

Bemarituzumab: Successes in Treatment of Gastric Cancer
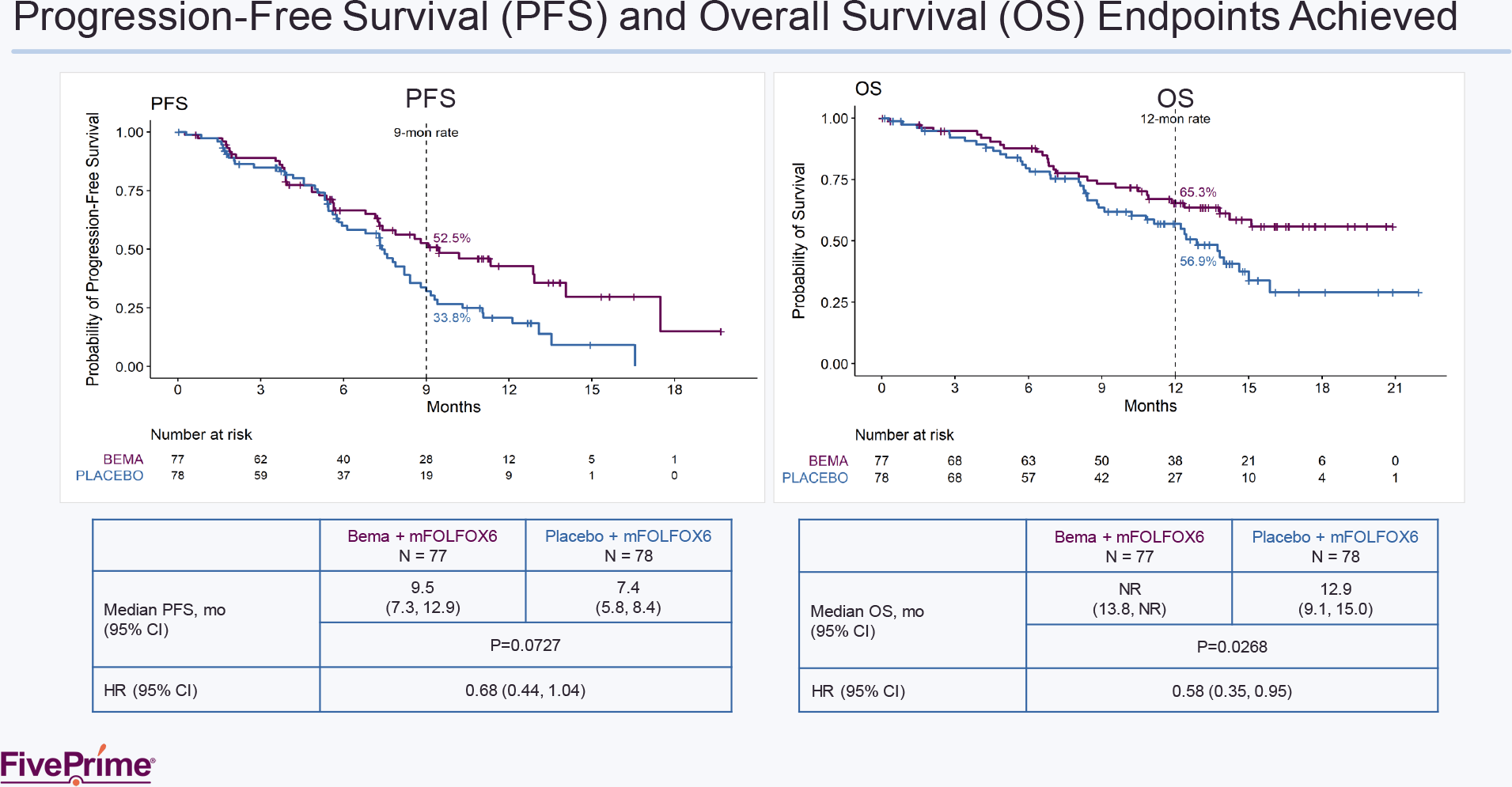
Bemarituzumab was fortunate in the FIGHT (NCT03694522) phase 2 clinical trial (randomized, double-blind, placebo-controlled, multicenter, international) involving adult patients (n=155) with previously untreated and inoperable (locally advanced or metastatic) cancer (adenocarcinoma) of the stomach or gastroesophageal junction. Subjects’ tumors had to be FGFR2b positive (FGFR2b overexpression and/or FGFR2 gene amplification) and negative for HER2.
Participants were administered either bemarituzumab on the background of the standard mFOLFOX6 regimen (leucovorin, fluorouracil, oxaliplatin) or the latter alone.
It has been demonstrated that the addition of bemarituzumab to standard treatment outperformed the latter alone:
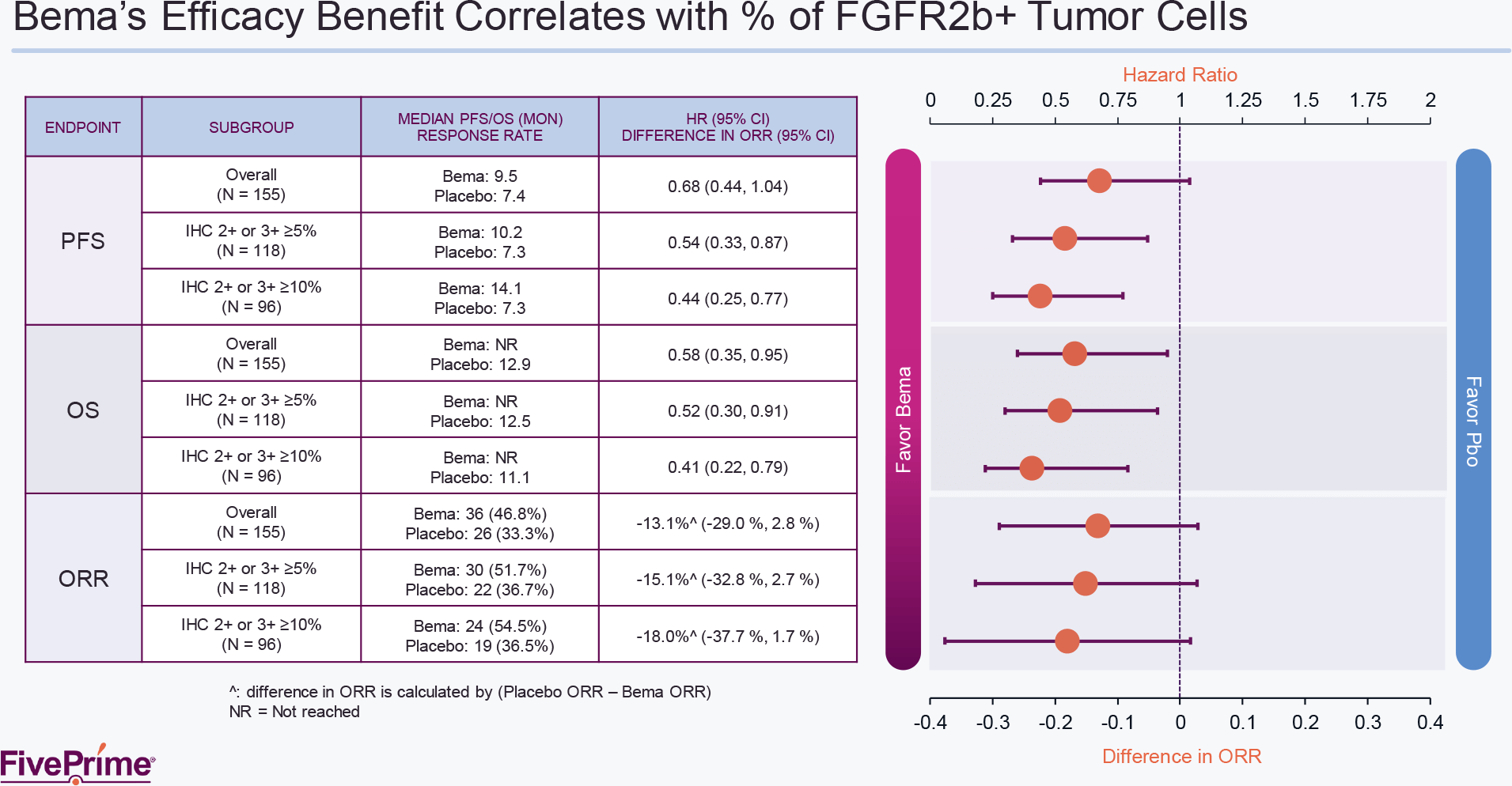
- overall response rate (ORR): 46.8% (n=36/77) — versus 33.3% (n=26/78) [p=0.106]
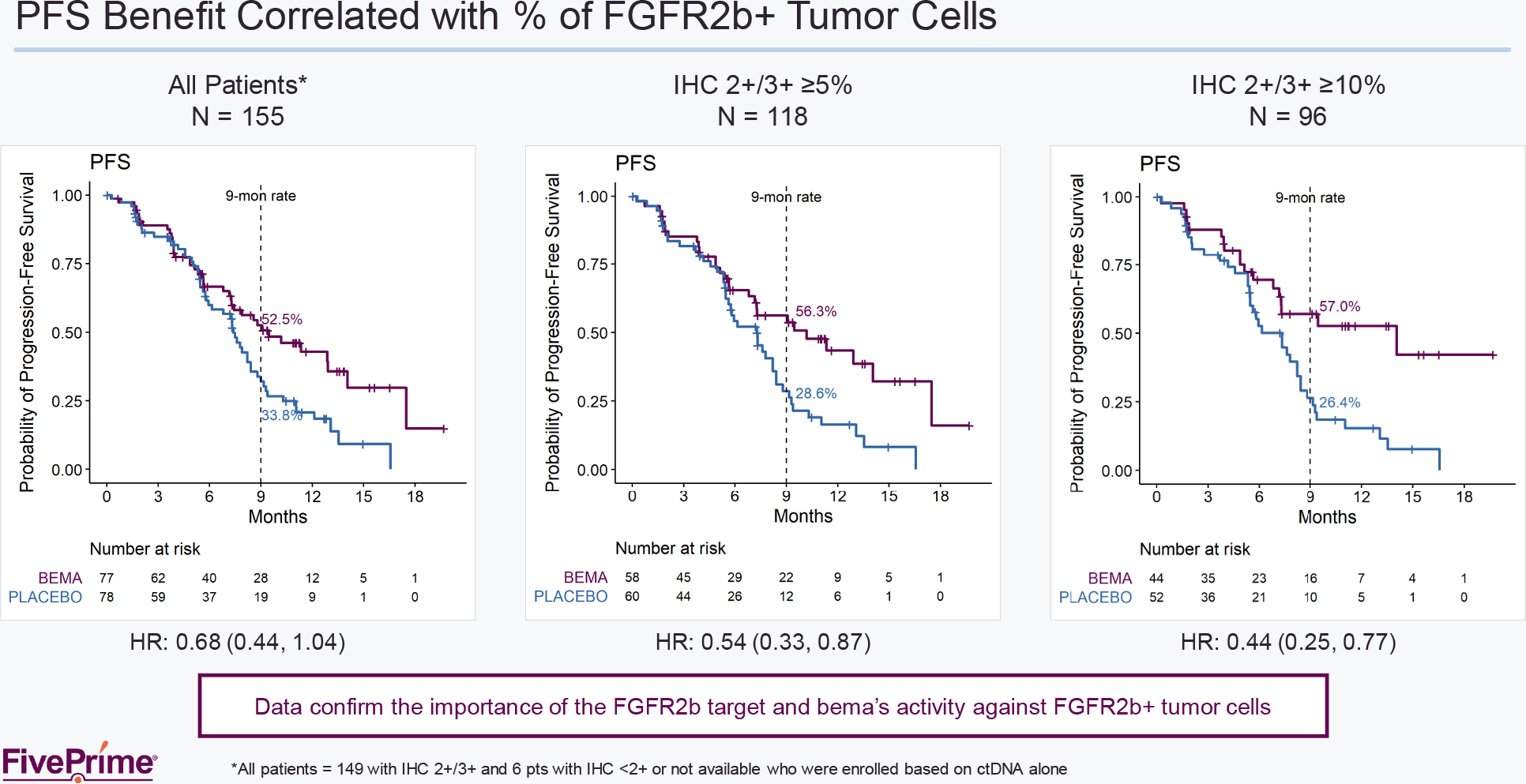
- median progression-free survival (PFS): 9.5 months — vs. 7.4 months (hazard ratio [HR] 0.68 [95% CI: 0.44–1.04]; p=0.073)
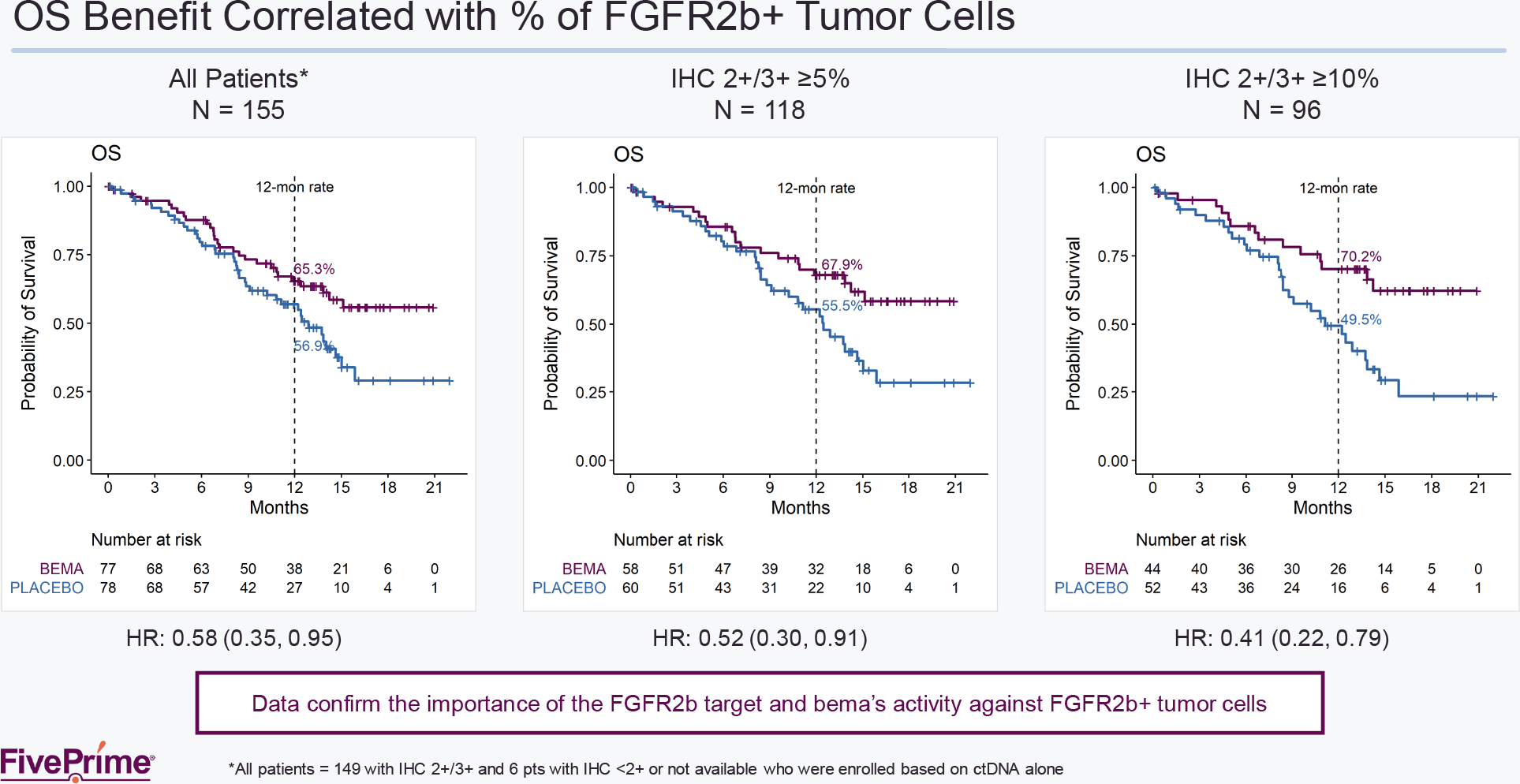
- median overall survival (OS): not yet reached — vs. 12.9 months (HR 0.58 [95% CI: 0.35–0.95]; p=0.027).
Important note: instead of the standard p-value of <0.05 indicating statistical significance, its threshold was set at <0.2. As FivePrime explained, the choice of such a strategy is justified by the fact that, first, the study is small and, second, it is still designed atypically for phase 2 (a strict design similar to a phase 3 randomized controlled trial [RCT]). In other words, the goal was to gain a deeper understanding of exactly who benefits from the experimental treatment.
When comparing the gastric cancer treatment outcomes provided by Herceptin (trastuzumab), an HER2 antagonist, or Opdivo (nivolumab), a PD-1 blocker, everything points in favor of bemarituzumab: both in terms of extending the disease progression-free period and in terms of reducing the risk of fatal outcome.

The only complaint about bemarituzumab was its safety profile: 67% of patients experienced corneal adverse events, such as dry eye (26% of patients), keratitis (16%), vision blurred (15%), punctate keratitis (15%), and corneal epithelium defect (11%) — versus 10% of participants in the control group.
No cases of retinal pigment epithelial detachment were observed, however. Corneal toxicity resolved in 60% of patients after a median of 22 weeks. Nevertheless, 22% of patients had to discontinue treatment with bemarituzumab because of corneal problems.
Bemarituzumab: Mechanism of Action
Bemarituzumab (FPA144) is a humanized monoclonal IgG1 antibody against fibroblast growth factor receptor 2b (FGFR2b, FGFR2IIIb). Bemarituzumab binds and inhibits FGFR2b on the surface of malignant cells thereby preventing FGFR2b from binding to its ligands, fibroblast growth factors 7, 10, and 22 (FGF7, FGF10, and FGF22), which promote tumor growth.

FGFR2b is a specific isoform of the receptor tyrosine kinase FGFR2 that is overexpressed in various types of cancer and is responsible for tumor proliferation, differentiation, and survival.
FGFR2b expression is observed, in addition to adenocarcinoma of the stomach or gastroesophageal junction (approximately 29% of cases), in non-small cell lung cancer (31%), triple-negative breast cancer (13%), ovarian cancer (40%), endometrial cancer (86%), cervical cancer (80%), colorectal cancer (62%), intrahepatic cholangiocarcinoma (22%), pancreatic cancer (4%).
Bemarituzumab induces antibody-dependent cell-mediated cytotoxicity (ADCC) against FGFR2b-expressing tumor cells. The result is inhibition of cell proliferation and apoptosis of malignant cells. Due to the modified glycosylation scheme (afucosylation) bemarituzumab exhibits increased affinity to Fc gamma receptor IIIA (FcγRIIIA, CD16a): since the latter is expressed by natural killer cells (NK cells) and macrophages, ADCC and local cytokine release processes are enhanced.

Notably, bemarituzumab does not inhibit the binding of fibroblast growth factor 23 (FGF23), which is responsible for phosphate and vitamin D metabolism. That is, there is no risk of hyperphosphatemia, which accompanies pan-FGF inhibitors.
Stomach Cancer: Just the Facts
- Stomach cancer affects more than 1 million people worldwide each year.
- Stomach cancer is the third leading cause of death from cancer, after lung cancer and breast cancer.
- Stomach cancer is the fifth most common cancer (excluding non-melanoma skin cancer) after lung, breast, prostate, and colon cancers.
- No first-line targeted therapy for stomach cancer has emerged in the past ten years. In October 2010, Herceptin (Herceptin, trastuzumab) was approved on a background of chemotherapy — for first-line therapy of HER2-positive metastatic stomach cancer or gastroesophageal junction cancer.
- Chemotherapy, proposed in the 1990s, is the standard treatment for 80–85% of patients with HER2-negative stomach cancer tumors.
- In countries without regular screening, up to 90% of stomach cancer diagnoses are made when the disease is at an advanced stage and is no more operable.
Five Prime Therapeutics: Drug Pipeline
Besides bemarituzumab, Five Prime has been developing other immuno-oncology experimental drugs. Yes, the incredible clinical success generated by the advent of PD-(L)1 and CTLA-4 blockers has made effective cancer treatment possible. Alas, many patients do not respond to these immune checkpoint inhibitors, and therefore there is a high unmet medical need for new drugs targeting other immunosuppressive mechanisms by which tumors evade immunological responses.

FPT155
FPT155 is a recombinant protein composed of the extracellular domain of soluble CD80 fused to a fragment crystallizable (Fc) region of human immunoglobulin G1 (IgG1). FPT155 has properties of immune stimulation, immune checkpoint inhibition, and antitumor activity.
CD80 (B7.1) is a costimulatory transmembrane protein expressed on activated antigen-presenting cells (APCs) involved in modulating T cell priming and activation, being a receptor for CD28 and CTLA4 on the T cell surface.
The CD80 motif of FPT155 targets and binds CD28, a protein expressed by nearly all CD4+ T helper cells and approximately half of CD8+ T killer cells, providing the costimulatory signals required for T cell activation and survival. Stimulation of T cells by CD28 and in the presence of antigenic T-cell receptor (TCR) signaling initiates costimulatory T cell responses, including naïve and memory T cell activation. This is reflected by the initiation of a cytotoxic T lymphocyte (CTL)-mediated anti-tumor immune response.
The CD80 motif of FPT155 also targets and binds cytotoxic T-lymphocyte-associated protein 4 (CTLA4, CD152) which is expressed by regulatory T cells and activated T cells and which, acting as an immune checkpoint, suppresses immune responses. CTLA4 is homologous to CD28, and both bind to CD80 and CD88 on APCs, with CTLA4 doing so with greater affinity and avidity than CD28 giving it a competitive binding advantage; as a result, CTLA4 inhibitory signals dominate CD28 stimulatory signals.

Binding of FPT155 to CTLA4 is reflected by the inhibition of the latter’s binding to endogenous CD80. This results in enhanced CD80–CD28 stimulatory interaction, CD28 signaling, and deregulation (reactivation) of T cells in the tumor microenvironment.
It should be understood that FPT155 is not a CD28 superagonist. At one time, the promising CD28 superagonist theralizumab, which does not require the presence of TCR, failed miserably: its use caused cytokine release syndrome in a severe life-threatening form. In addition, FPT155, unlike Yervoy (ipilimumab), CTLA4 blocker by Bristol-Myers Squibb, triggers activation and proliferation of even those T-cells that do not express CTLA4. It is believed that the activity of the soluble CD80 motif of FPT155 is comparable or superior to that of other T-cell agonists such as GITR, OX40, and 4-1BB ligands.
The NCT04074759 phase 1 clinical trial is testing FPT155 alone and in combination with Keytruda (pembrolizumab), a PD-1 blocker from Merck & Co., in the treatment of advanced solid tumors that are inoperable, locally advanced or metastatic and have progressed after all courses of standard therapy or are unfit for such therapy. The synergy between the mechanisms of action of FPT155 and pembrolizumab is thought to be worthwhile: Bristol-Myers Squibb has repeatedly proven the reasonableness of the combination of the PD-1 blocker Opdivo (nivolumab) and Yervoy.
FPA157
FPA157 is a monoclonal antibody against CCR8 that enhances antibody-dependent cell-mediated cytotoxicity (ADCC) and causes natural killer (NK)-mediated destruction of target cells — to eliminate predominantly regulatory T cells (Tregs) CCR8+ from the tumor microenvironment.
Regulatory T cells suppress immune responses in the tumor microenvironment through a variety of suppressive mechanisms. Systemic drugs targeting Tregs lack specificity to intratumor Tregs and can deplete the pool of effector cells thereby upsetting the balance: a critical role of Tregs is to maintain immune homeostasis and prevent autoimmune responses.

C-C motif chemokine receptor 8 (CCR8) is a chemokine receptor that is selectively expressed on activated intratumor Tregs and is essential for one of the Tregs CCR8+-mediated immunosuppression mechanisms. High levels of the latter in cancer correlate with immune tolerance, poor overall survival, and insufficient therapeutic response to chemotherapy drugs.
BMS-986258
BMS-986258 is a monoclonal antibody against TIM-3 that has anti-tumor immune checkpoint inhibitor properties. It is a collaborative project with Bristol-Myers Squibb.
T-cell immunoglobulin and mucin-domain containing-3 (TIM-3, HAVCR2) is a transmembrane protein expressed on type 1 T helper (Th1) CD4+ interferon gamma (IFNγ)-producing and type 1 T cell (Tc1) as well as on Tregs and immunocytes of the innate immune system (dendritic cells, natural killer cells, monocytes), which is a negative regulator of their functions. Overexpression of TIM-3 in various types of cancer has been observed.
Binding of BMS-986258 to TIM-3, which acts as an inhibitory immune checkpoint, disables T cell suppression, activates antigen-specific T lymphocytes and enhances CTL-mediated lysis of tumor cells, which is reflected in tumor growth inhibition.

BMS-986258 is in phase 1/2 clinical trial NCT03446040 for the treatment of renal cell carcinoma, colorectal cancer, non-small cell lung cancer, head and neck squamous cell carcinoma, triple-negative breast cancer that has progressed or recurred after at least one line of therapy for disseminated or metastatic indications; or if patients have experienced intolerance of such therapy. BMS-986258 is studied monotherapeutically and in combination with Opdivo or recombinant human hyaluronidase PH20 (rHuPH20).
Expert Notes
The purchase of Five Prime is indicative of Amgen’s desperate position in the field of developing cancer drug compounds. On its experimental pipeline only sotorasib (AMG 510), focused on the therapy of KRASG12C-mutant non-small cell lung cancer, is awaiting regulatory approval. The remaining molecules are in the early stages of clinical trials.
Amgen does not often invest in large-scale acquisitions of any promising assets as other Big Pharma players do. Between 2011 and 2013, for example, it spent more than $12 billion to acquire Bayovex, Micromet, and Onyx Pharmaceuticals. The first brought the oncolytic virus Imlygic (talimogen laherparepvec) against melanoma, the second provided Blincyto (blinatumomab) against CD19-positive B-cell precursor acute lymphoblastic leukemia (B-ALL), a third gave the anti-myeloma drug Kyprolis (carfilzomib) and opened access to a number of collaborations with other pharma companies, including the oncology drugs Nexavar (sorafenib), Stivarga (regorafenib), Ibrance (palbociclib).
In 2019, Amgen acquired a 20% stake in China’s BeiGene and shelled out $13.4 billion for Otezla (apremilast) against autoimmune diseases.
It’s hard to believe that not long ago, FivePrime was in extreme distress when its stock price had been gradually deteriorating since the fall of 2017 eventually losing 90% in three years. The problem was the failure of cabiralizumab, a joint with Bristol-Myers Squibb monoclonal antibody against the colony stimulating factor 1 receptor (CSF1R). Such a mechanism of action was expected to block macrophage activation and survival providing a reduction in the population of immunosuppressive tumor-associated macrophages (TAMs) in the tumor microenvironment thereby enhancing the immune response to malignant cells.

Because Five Prime partnered with China’s Zai Lab in December 2017, granting it an exclusive license to sell bemarituzumab, Amgen’s wallet will be filled with good royalties, as China has one of the highest rates of gastric cancer in the world.
Amgen is independently working on two drug candidates against gastric cancer: BiTE antibodies AMG 199 and AMG 910. The first targets mucin 17 (MUC17) and the second targets claudin-18 isoform 2 (CLDN18.2).
Nevertheless, Five Prime should explain why the upper limit of the confidence interval for PFS was above 1.0 and how critical it is that 34% of patients in the bemarituzumab group discontinued treatment because of adverse events (versus 5% in the control group).
In addition, nothing is said about the baseline characteristics of the subjects: perhaps the imbalance of the patient population between the experimental therapy and standard treatment groups contributed to the success of bemarituzumab.
Moreover, PD-1 blockers Opdivo and Keytruda are beginning to take priority in the treatment of gastric, gastroesophageal junction, and esophageal cancer: at any rate, their addition to first-line standard chemotherapy prolongs patients’ lives.
Extras
Five Prime Therapeutics: rewriting cancer, together. February 2021. [PDF]
A double-blind randomized study of bemarituzumab (bema) plus mFOLFOX6 versus placebo plus mFOLFOX6 as first-line treatment for advanced gastric/gastroesophageal junction cancer (FIGHT). January 16, 2021. [PDF]
Five Prime Therapeutics. Corporate overview. November 2020. [PDF]
Bemarituzumab. Targeted therapy for FGFR2b+ tumors. November 10, 2020. [PDF]
FPT155, a novel therapeutic CD80-Fc fusion protein, with potent anti-tumor activity in preclinical models. [PDF]
A phase 1 study of FPT155, a first-in-class CD80 extracellular domain-Fc fusion protein, in patients with advanced solid tumors. [PDF]
Development of FPA157, an anti-CCR8 depleting antibody engineered to preferentially eliminate tumor-infiltrating T regulatory cells. [PDF]