WHAT HAPPENED
Datroway/Datverzo (datopotamab deruxtecan) is a new drug indicated for the treatment of locally advanced or metastatic nonsquamous non-small cell lung cancer (NSCLC) in adult patients who have previously received systemic therapy.
In the fourth quarter of 2024, the U.S. Food and Drug Administration (FDA) will make a decision regarding the approval of Datroway/Datverzo [1].
The European Medicines Agency (EMA) is also reviewing the marketing authorization application (MAA) for Datroway/Datverzo for the treatment of locally advanced or metastatic nonsquamous NSCLC in adult patients who require systemic therapy following prior treatment [2].
AstraZeneca and Japan’s Daiichi Sankyo are behind the development of datopotamab deruxtecan: the former is responsible for the commercialization of the drug worldwide, except Japan, where the latter is in charge.
Datroway is a hypothetical brand name for datopotamab deruxtecan. The presumed alternative brand name is Datverzo. There are several variants of developments:
- Datopotamab deruxtecan will be marketed under different brand names in different regions.
- If one brand name for datopotamab deruxtecan cannot be successfully trademarked and registered in a country, a second one will be used.
- Since datopotamab deruxtecan also expects to seek regulatory approval for the treatment of HR+/HER2− breast cancer, in this indication it may be marketed under a brand name different from the one chosen for NSCLC.

WHY IT MATTERS
Lung cancer is one of the most common cancers and the leading cause of malignancy-related deaths globally [1] [2] [3]. Non-small cell lung cancer (NSCLC) is the most common type of lung cancer (85%–90% of cases), with at least half of cases diagnosed at advanced or metastatic stage [4] [5] [6] [7] [8]. In around 70%–75% of NSCLC cases, tumors exhibit nonsquamous cell histology [9] [10] [11] [12].
Although immunotherapy (with optional chemotherapy) and targeted therapies have significantly improved clinical outcomes in the first-line treatment of NSCLC, most patients experience disease progression sooner or later. Even if NSCLC is diagnosed early and treated in time, half of patients still progress to the metastatic stage within five years. Chemotherapy administered in second and subsequent lines of therapy is characterized by limited efficacy along with toxicity [13] [14] [15] [16] [17] [18]. This is why new drugs are needed.
WHAT IT FOUND OUT
The ongoing TROPION-Lung01 (NCT04656652) phase 3 (randomized, open-label, active-controlled, multicenter, international) is evaluating the efficacy and safety of datopotamab deruxtecan versus docetaxel in the treatment of locally advanced or metastatic non-small cell lung cancer (NSCLC) regardless of the presence or absence of genomic alterations (EGFR, ALK, ROS1, ROS1, NTRK, BRAF, MET, or RET) in adult patients who have previously received at least one prior line of systemic therapy.
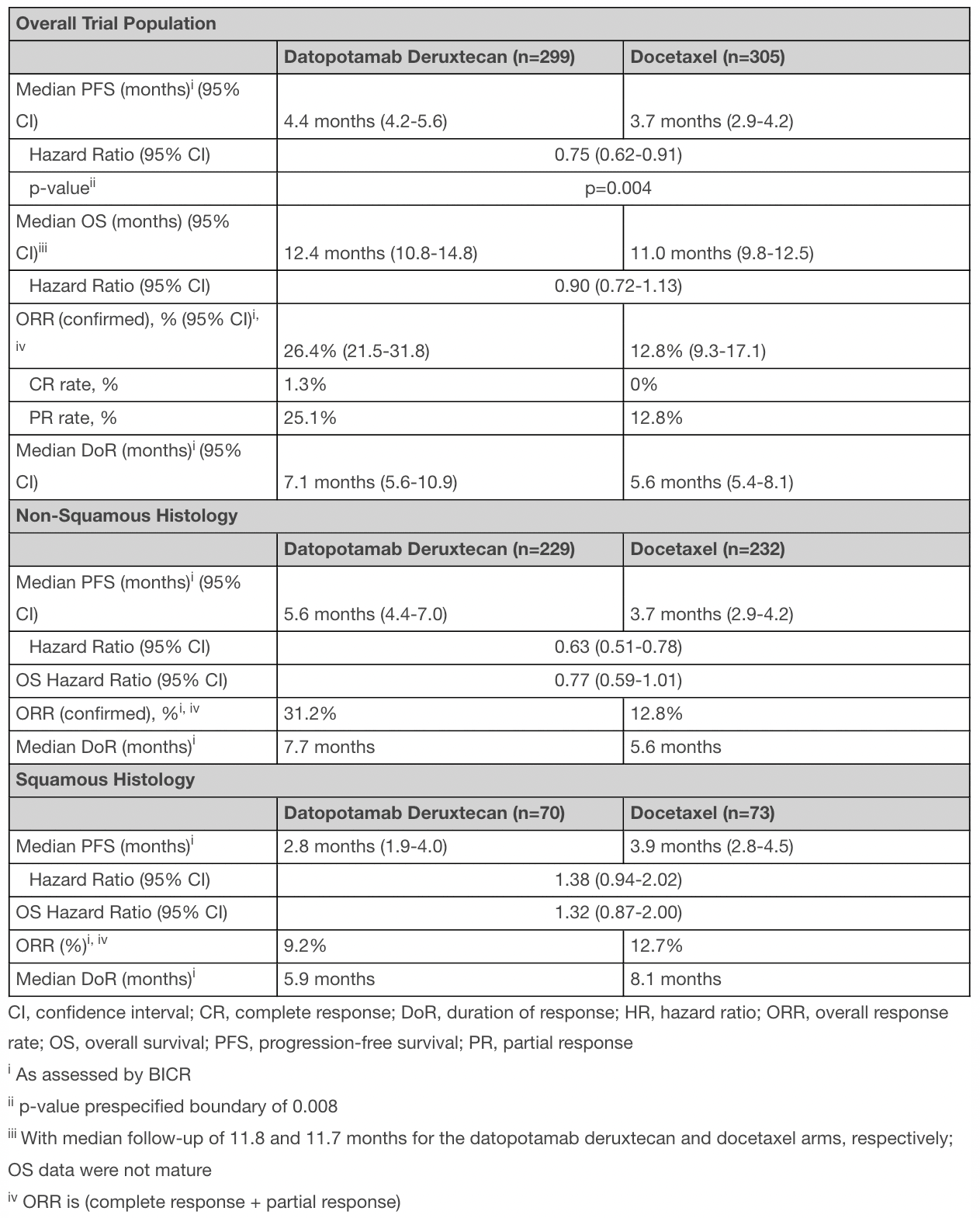
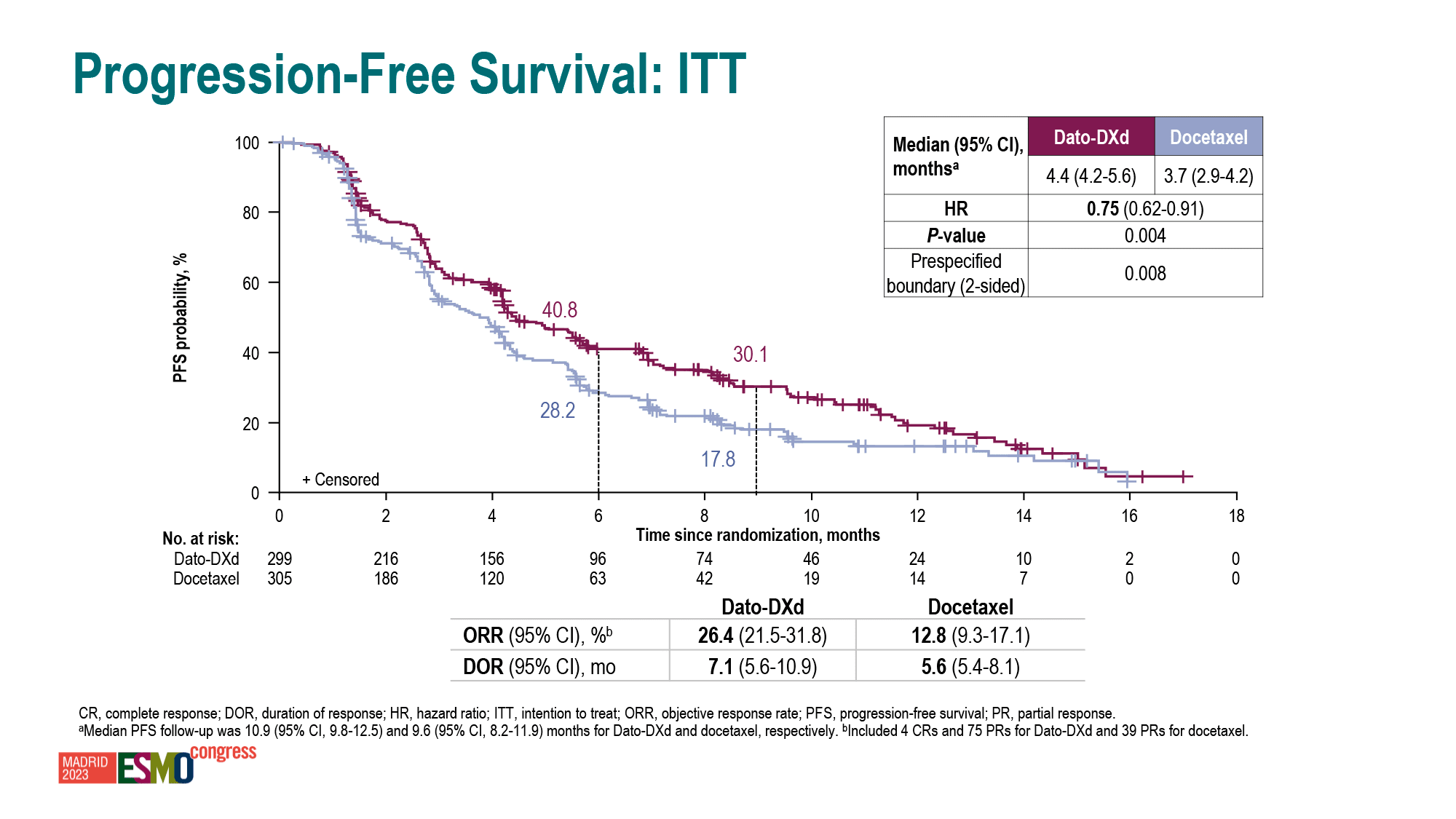
According to the interim results, datopotamab deruxtecan provided a 25% reduction in the risk of disease progression or death relative to docetaxel: hazard ratio (HR) 0.75 (95% CI [hereafter]: 0.62–0.91; p=0.004). Median progression-free survival (PFS) came out to 4.4 months (4.2–5.6) — versus 3.7 months (2.9–4.2) [1].
The overall response rate (ORR) was 26% (22–32), including 1.3% complete response (CR) and 25% partial response (PR) — vs. 13% (9–17), including 0% CR and 13% PR. The median duration of response (DoR) was 7.1 months (5.6–10.9) — vs. 5.6 months (5.4–8.1).
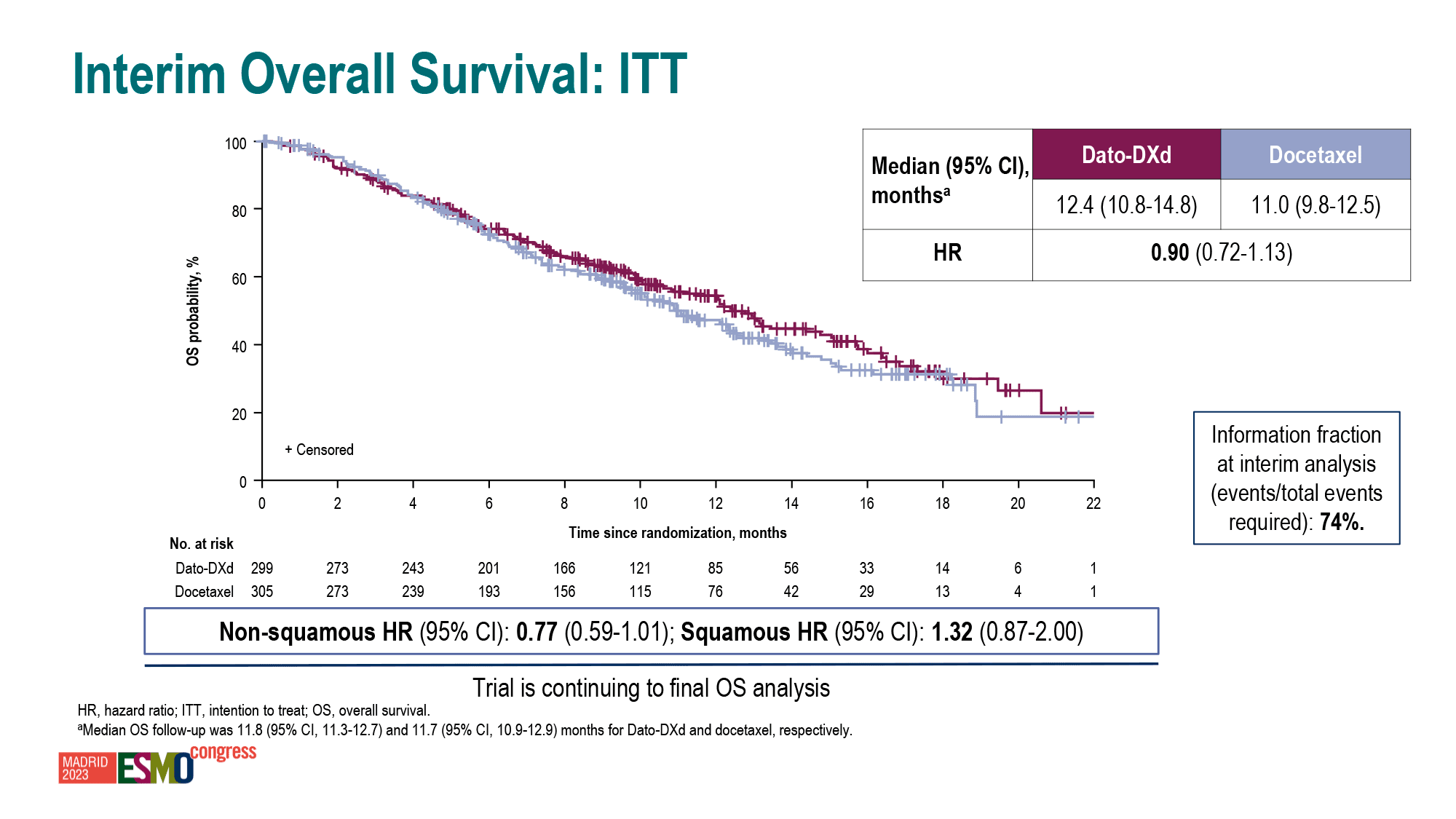
The median overall survival (OS) has not yet matured, but in the datopotamab deruxtecan group has already numerically surpassed that in the docetaxel group: HR 0.90 (0.72–1.13).
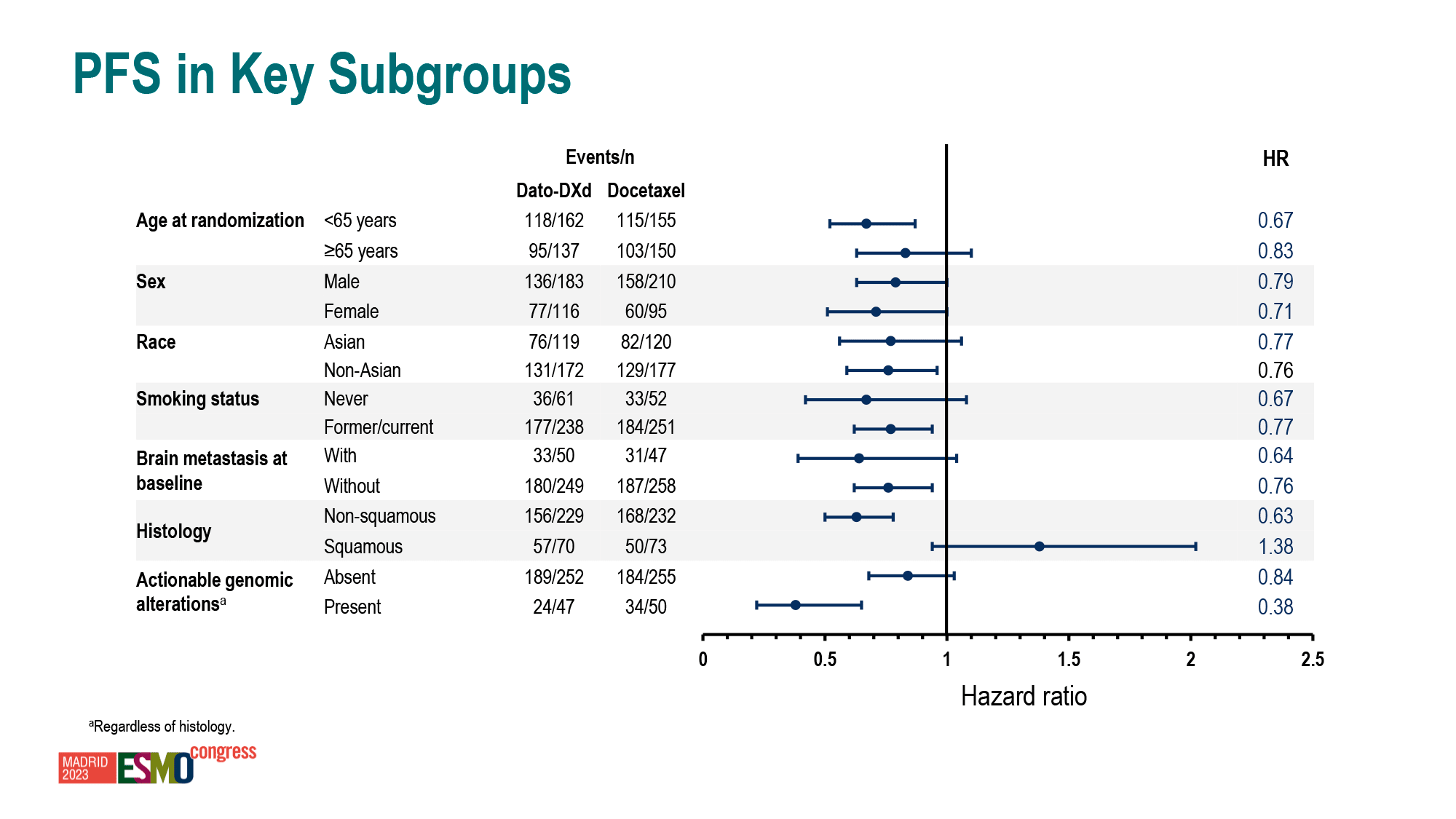
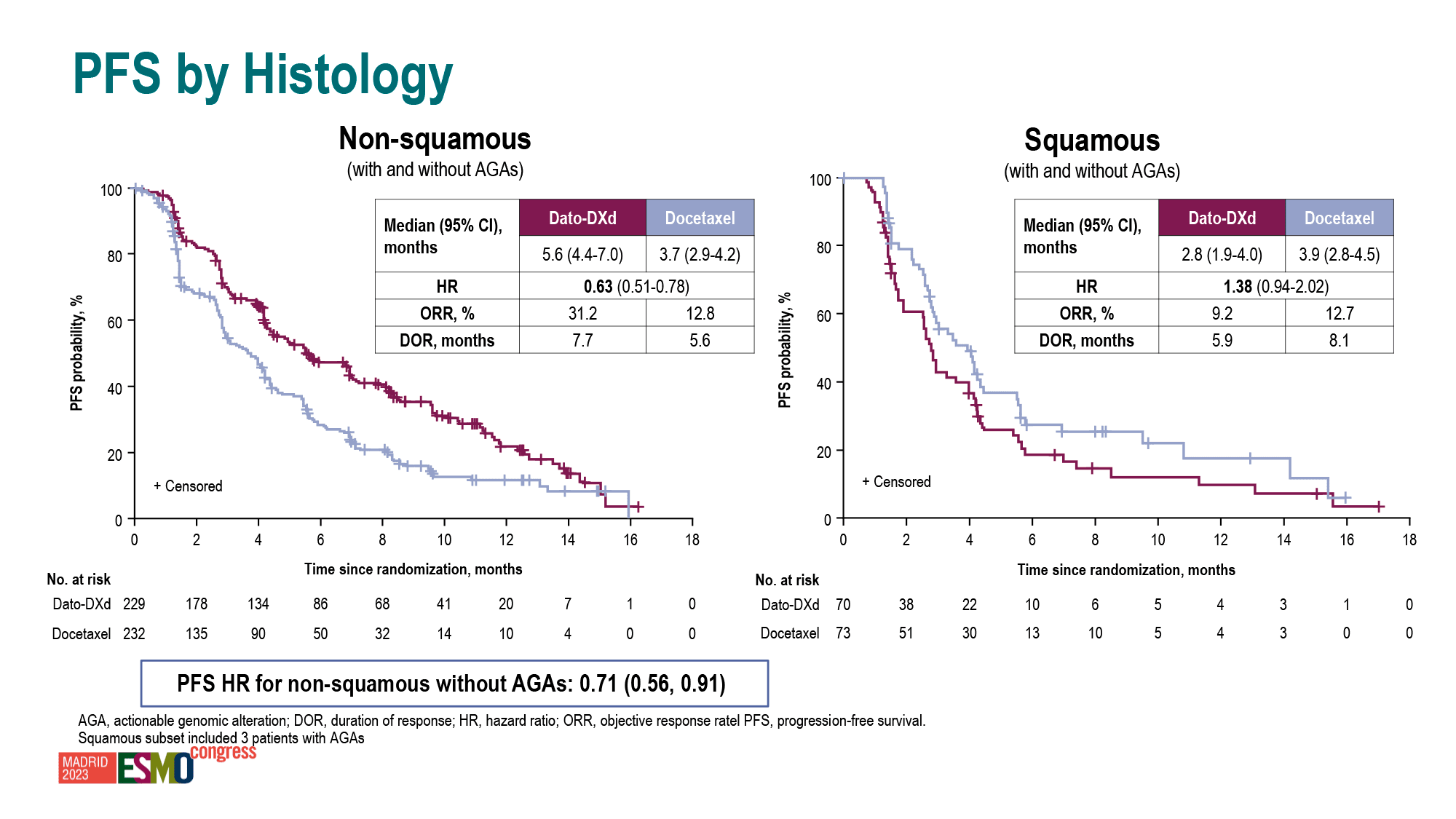
Subjects with nonsquamous histology had better clinical outcomes than those with squamous one: PFS HR 0.63 (0.51–0.78) vs. 0.71 (0.56–0.91), ORR 31% vs. 9%, DoR 7.7 months vs. 5.9 months, OS HR 0.77 (0.59–1.01) vs. 1.32 (0.87–2.00).
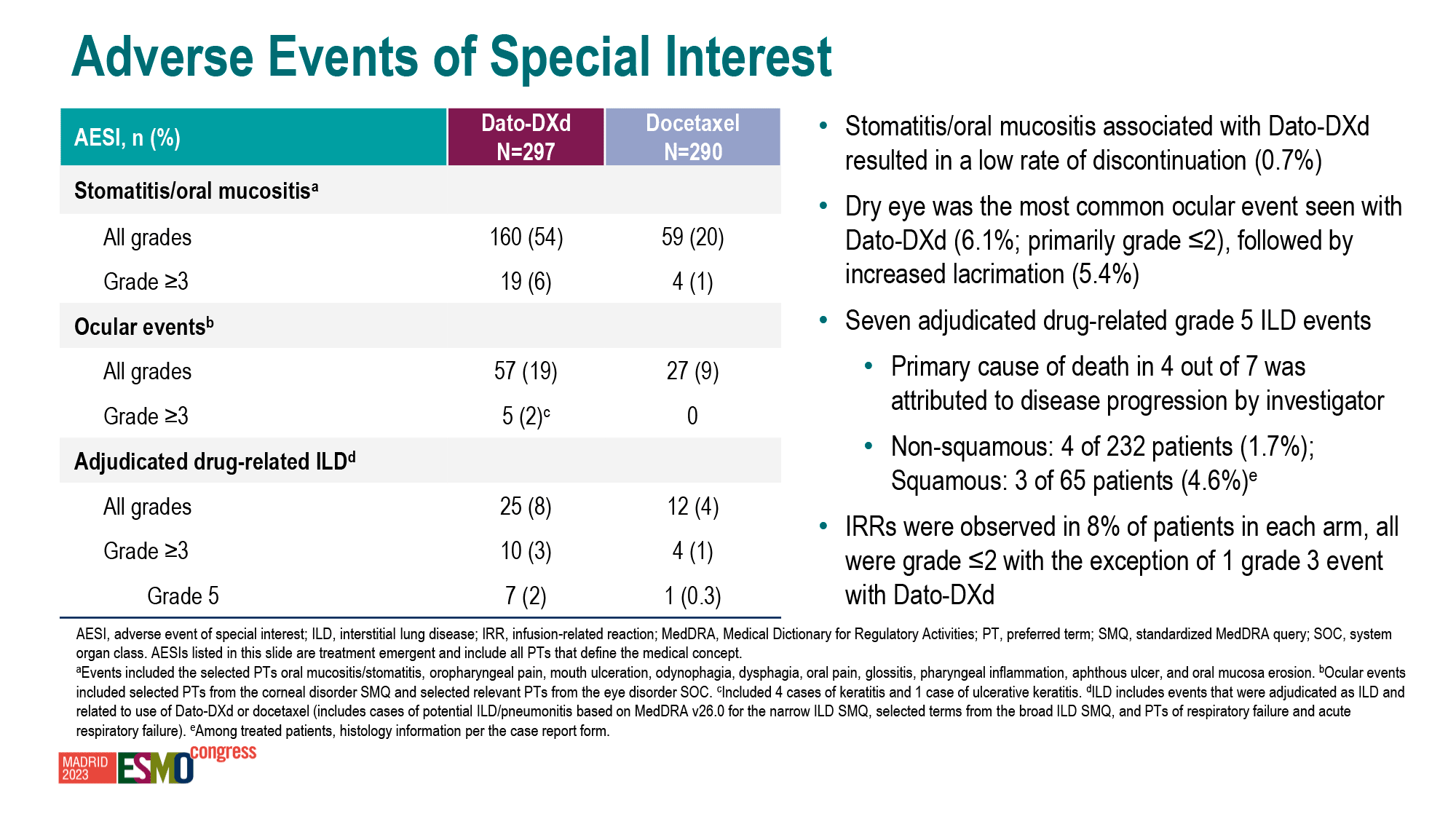
The administration of datopotamab deruxtecan was accompanied by interstitial lung disease (ILD), an adverse event of special interest (AESI) when using antibody–drug conjugates [2]. Grade 3 or higher ILD events occurred in 3% of patients.
THE ESSENCE
The therapeutic efficacy of Datroway/Datverzo (datopotamab deruxtecan) appears to be very weak, with only negligible improvement in clinical outcomes compared to docetaxel. While the relative differences were statistically significant, the absolute prolongation of progression-free survival (PFS) is minuscile. Unfortunately, datopotamab deruxtecan did not provide the great advancement that was hoped for. Therefore, there are doubts as to whether the approval of this drug is justified for the treatment of locally advanced or metastatic NSCLC. This is because the cost of this drug will be dramatically higher than that of the common docetaxel, which lost its patent protection in 2010 and is now available in generic form.

Not All Cancer Drugs Are Equally Useful
Cheating out of ignorance, or Sleight of hand and no fraud. How pharmaceutical companies scam clinical trials.
However, we should wait for the final results of the clinical trial. The overall survival (OS) data may change the pessimistic view, particularly if certain patient subpopulations benefit from a clear and distinct advantage.
It is important to note that docetaxel (with optional ramucirumab) has been the primary drug for second-line therapy of progressive advanced NSCLC for many years [1] [2]. Although many therapies have attempted to outperform it, they have failed.
HOW IT WORKS
Datopotamab deruxtecan (Dato-DXd) is an antibody–drug conjugate (ADC) composed of a humanized IgG1 monoclonal antibody against TROP2 and a cytotoxic drug load DXd combined by a stable linker.
Trophoblast cell surface protein 2 (TROP2), also known as tumor-associated calcium signal transducer 2 (TACSTD2), is overexpressed in many types of epithelial cancers and is associated with enhanced tumor aggressiveness, metastasis, drug resistance, and increased tumor cell survival [1] [2] [3].
After TROP2-expressing tumor cells internalize datopotamab deruxtecan, their lysosomal enzymes cleave the tetrapeptide-based covalent linker, resulting in the cytoplasmic release of DXd, a derivative of exatecan (DX-8951), a topoisomerase I inhibitor. After entering the cell nucleus, DXd damages DNA, thereby inducing cell death (apoptosis). After lysis of the dead tumor cells, DXd, characterized by high cell membrane permeability, penetrates into neighboring tumor cells, eventually killing them, regardless of TROP2 expression (i.e. bystander antitumor effect). Due to the short half-life of DXd, the risk of systemic toxicity is reduced [4] [5] [6] [7] [8].
In fact, datopotamab deruxtecan represents a dramatically improved version of conventional chemotherapy and is therefore appropriately positioned as a biologically targeted chemotherapy.
WHAT’S NEXT
Datroway/Datverzo (datopotamab deruxtecan) anticipates significantly expanding the population of eligible patients with NSCLC over time. To this end, AstraZeneca and Daiichi Sankyo are conducting a large-scale phase 3 clinical program for the use of datopotamab deruxtecan in the first-line treatment of locally advanced or metastatic NSCLC.
The design of the clinical trials is based on a number of statements. Thus, according to preclinical data, the combination of datopotamab deruxtecan and PD-(L)1 blocker is characterized by enhanced antitumor activity than separately [1]. The use of PD-(L)1 blockers with optional chemotherapy prolongs survival, but the 5-year survival rate is still low [2] [3] [4], especially when PD-L1 expression level is insufficient [5] [6] [7] [8], and such a pattern is due to the development of resistance to treatment with these immune checkpoint inhibitors (ICIs) [9]. Be that as it may, it is necessary to elucidate which subpopulation of patients is best served by the combination of immunotherapy with datopotamab deruxtecan.
- AVANZAR (NCT05687266), squamous and nonsquamous NSCLC without genomic alterations, TROP2-positive: Datroway/Datverzo + Imfinzi (durvalumab) + carboplatin — versus Keytruda (pembrolizumab) + chemotherapy.
- TROPION-Lung07 (NCT0555555732), nonsquamous NSCLC without genomic alterations, PD-L1 expression < 50%: Datroway/Datverzo + Keytruda ± platinum-based chemotherapy — vs. Keytruda + pemetrexed + platinum-based chemotherapy.
- TROPION-Lung08 (NCT05215340), squamous and nonsquamous NSCLC without genomic alterations, PD-L1 expression ≥ 50%: Datroway/Datverzo + Keytruda — vs. Keytruda.
In general, a global goal has been set: Datroway/Datverzo should replace conventional chemotherapy for as many different types of cancer as possible.
WHAT’S MORE
Datroway/Datverzo (datopotamab deruxtecan) also hopes to secure regulatory approval in the treatment of breast cancer.
The TROPION-Breast01 (NCT05104866) phase 3 (randomized, open-label, active-controlled, multicenter, international) clinical trial demonstrated that datopotamab deruxtecan improved, vs. chemotherapy, outcomes for unresectable or metastatic hormone receptor positive (HR+) and HER2 low or negative (HER2–) [IHC 0, IHC 1+ or IHC 2+/ISH–] breast cancer in adult patients who had previously received endocrine therapy and at least one line of systemic therapy.
The administration of datopotamab deruxtecan resulted in a 37% reduction in the risk of disease progression or death by 37% compared to chemotherapy: HR 0.63 (0.52–0.76; p<0.0001). Median PFS was 6.9 months (5.7–7.4) vs. 4.9 months (4.2–5.5), ORR was 36% vs. 23%. The median OS was not yet mature but numerically superior: HR 0.84 (0.62–1.14) [1].
MEANWHILE
Datroway/Datverzo (datopotamab deruxtecan) is not the first drug targeting TROP2.
In late April 2020, Immunomedics, acquired by Gilead Sciences for $21 billion in late October of that year [1], launched Trodelvy (sacituzumab govitecan), an antibody–drug conjugate (ADC) with exactly the same mechanism of action, for the treatment of triple-negative breast cancer [2] [3]. More recently, sacituzumab govitecan has hooked up the treatment of HR+/HER2− breast cancer and urothelial cancer [4] [5].
In late January 2024, Gilead announced that Trodelvy did not statistically outperform docetaxel in improving overall survival (OS) in a clinical trial of a second-line treatment for metastatic NSCLC. The results are expected to be similar weak to those of Datroway/Datverzo. However, clinical development is ongoing, and sacituzumab govitecan may prove effective for certain patient subpopulations [6].
The therapeutic efficacy of Trodelvy against inoperable or metastatic HR+/HER2− breast cancer is similar to that of Datroway/Datverzo, both of which are equally low. This is expected due to the incurable nature of the disease at this stage.