Highlights
Vabysmo (faricimab) is a new drug indicated to treat patients with neovascular (wet) age-related macular degeneration (AMD) or diabetic macular edema (DME).
Vabysmo, developed by Roche, is approved by the U.S. Food and Drug Administration (FDA) in late January 2022.
The European Medicines Agency (EMA) continues to examine the application for faricimab.
A key marketing advantage of Vabysmo over other drugs commonly used in ophthalmic practice for the indicated diseases lies in the possibility of more infrequent dosing. The scheme of prescribing faricimab assumes several loading doses monthly with subsequent doses of the drug every 2, 3, or 4 months; the interval depends on the disease activity and fixation of the proper therapeutic effect. Given that all such medications are administered by intraocular injection (intravitreal), less frequent use of Vabysmo will have a less traumatic effect on the eyes. As a result, patients will be more willing to adhere to treatment, which will be properly reflected in the inhibition of disease progression.

Vabysmo: Mechanism of Action of Faricimab
Faricimab (RG7716, RO6867461) is a bispecific monoclonal antibody that binds and inactivates both vascular endothelial growth factor A (VEGF-A) and angiopoietin-2 (Ang2).
VEGF-A inhibition leads to suppression of endothelial cell proliferation, neovascularization, and vascular permeability. Ang2 inhibition promotes vascular stability and desensitization to the action of VEGF-A.
Administered intravitreally, faricimab is developed by Genentech, part of Roche, and Japan’s Chugai Pharmaceutical, in which the Swiss pharmaceutical giant holds a majority stake.
Vabysmo: Efficacy of Faricimab for Neovascular Age-Related Macular Degeneration
Identical in design, the TENAYA (NCT03823287) and LUCERNE (NCT03823300) phase 3 (randomized, double-blind, active-controlled, multicenter, international) clinical trials invited adult (50 years and older) patients (n=1329) with previously untreated choroidal neovascularization (CNV) secondary to neovascular age-related macular degeneration.
Participants received faricimab (every 2, 3, or 4 months after 4 monthly loading doses) or aflibercept (every 2 months after 3 monthly loading doses).
After 48 weeks of treatment, it was documented that 45% of patients in the Vabysmo group showed, according to optical coherence tomography and visual acuity assessment, a 4-month interval between doses of the drug, 33% of subjects showed a 3-month interval, and the remaining 22% showed a 2-month interval. This, however, does not mean that such a proportional distribution of the faricimab dosing regimen would be unconditionally fair in clinical practice: everything depends on the course of the disease in each individual patient.
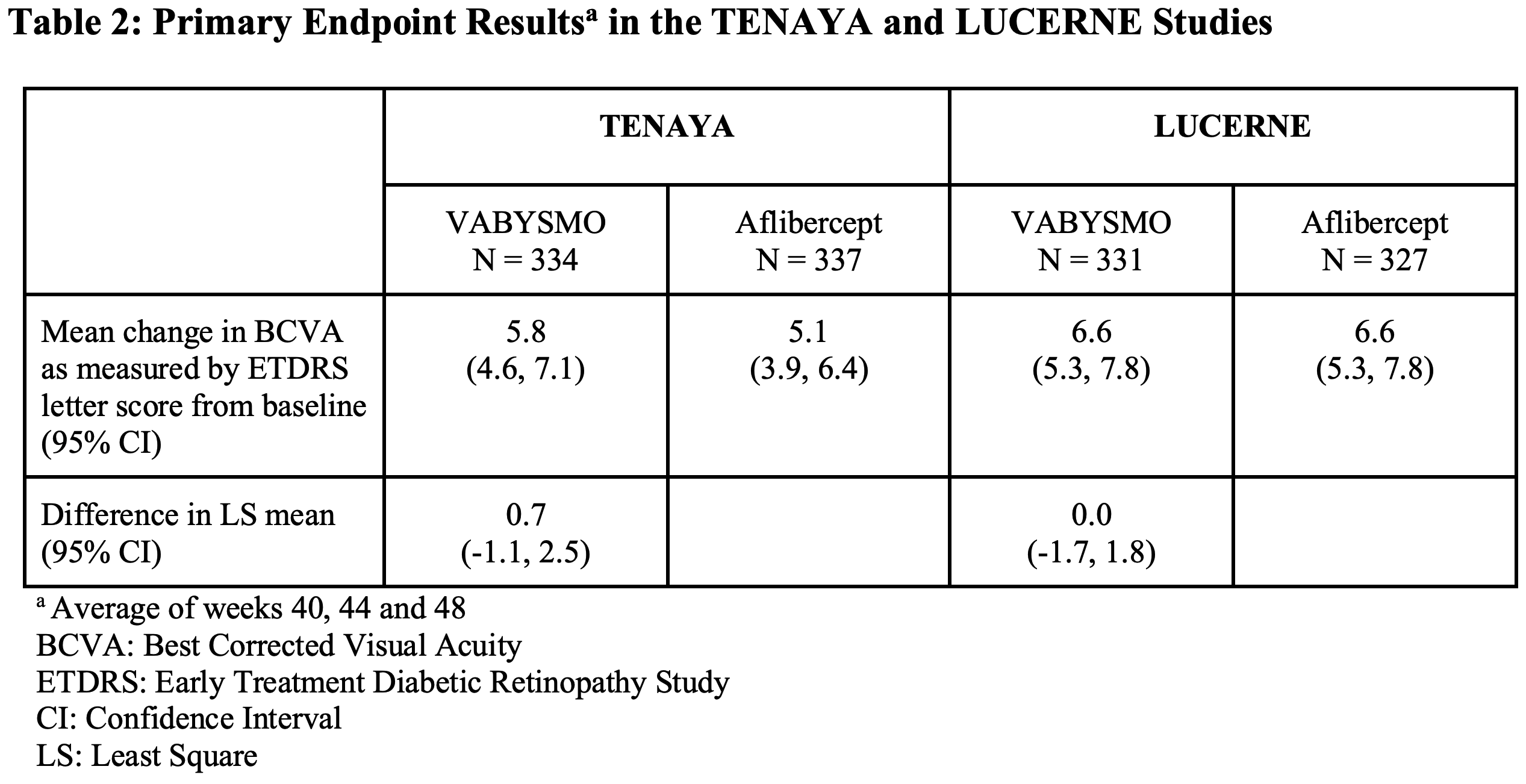
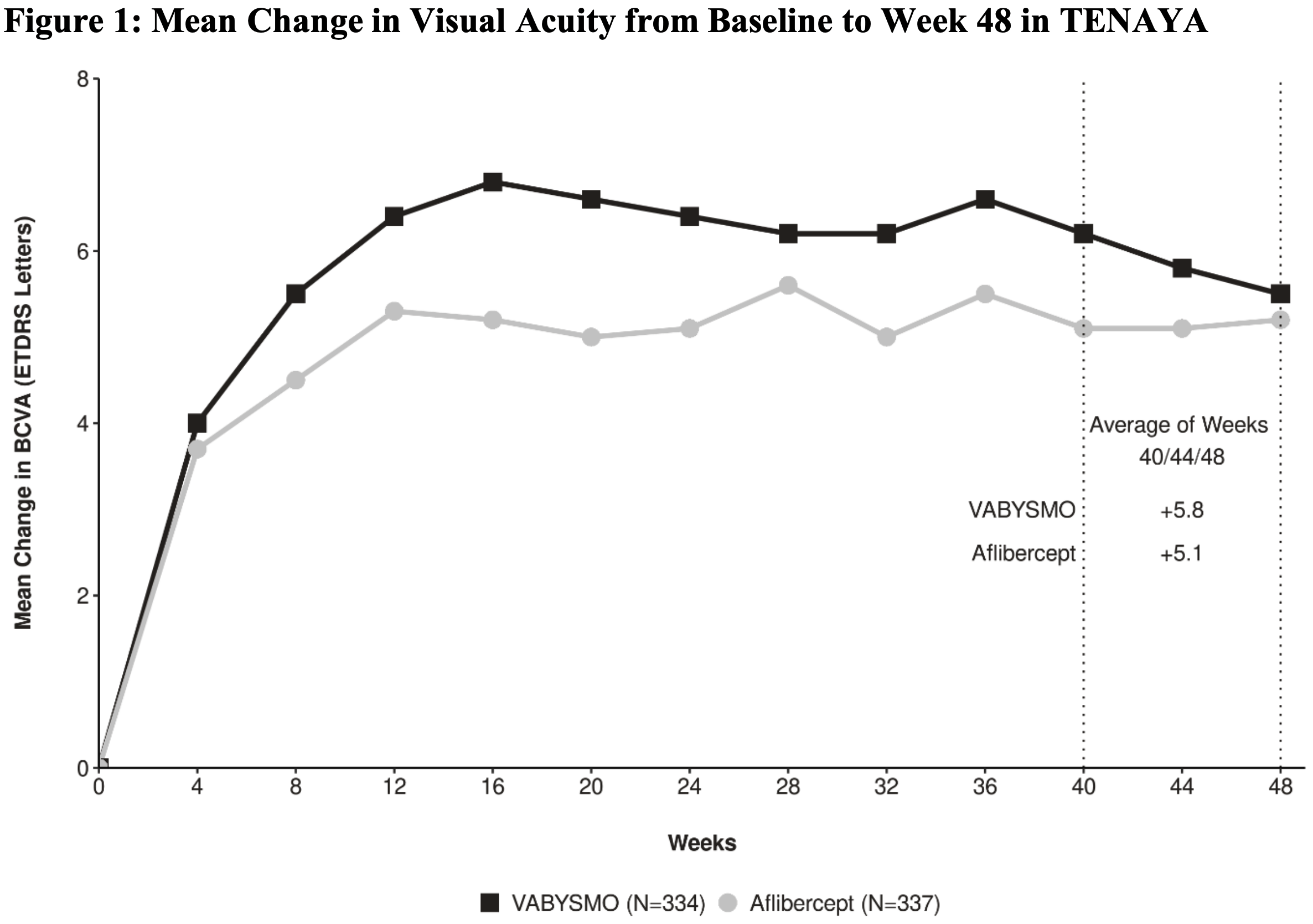
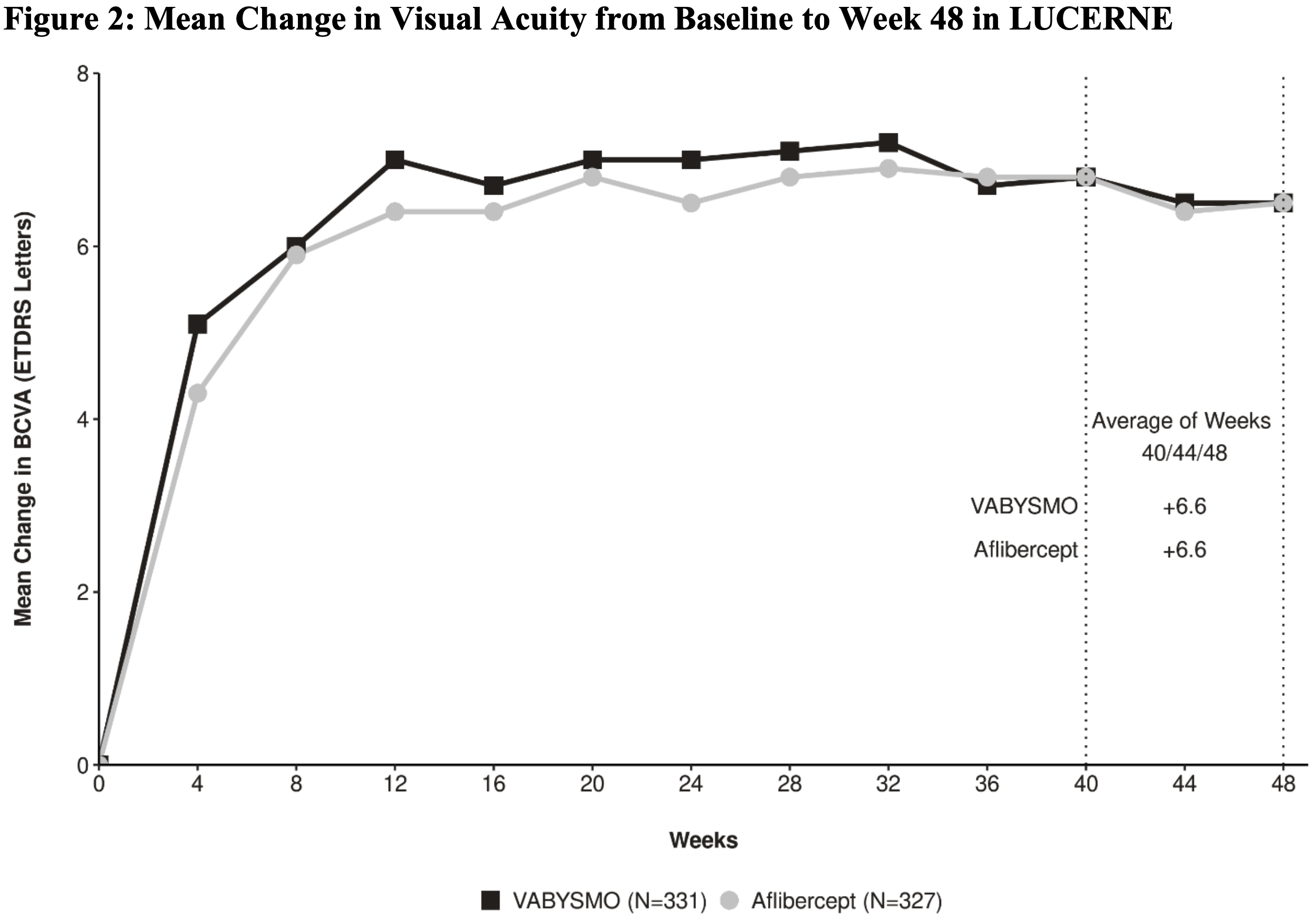
The primary endpoint of treatment efficacy was the change in Best-Corrected Visual Acuity (BCVA) averaged over 40, 44, and 48 weeks of therapy, according to the Early Treatment Diabetic Retinopathy Study (ETDRS) letter chart.
Vabysmo was found to be no worse than Eylea: respectively in TENAYA and LUCERNE, the mean change in BCVA was 5.8 (95% CI: 4.6–7.1) and 6.6 (95% CI: 5.3–7.8) letters in the faricimab groups — versus 5.1 (95% CI: 3.9–6.4) and 6.6 (95% CI: 5.3–7.8) letters in the aflibercept groups.
Vabysmo: Efficacy of Faricimab for Diabetic Macular Edema
Identical in design, the YOSEMITE (NCT03622580) and RHINE (NCT03622593) phase 3 (randomized, double-blind, active-controlled, multicenter, international) clinical trials invited adult (18 years and older) patients (n=1891) with macular thickening secondary to diabetic macular edema involving the center of the fovea.
Patients had to have type 1 or type 2 diabetes mellitus (glycated hemoglobin [HbA1c] level ≤ 10%) and the decrease in visual acuity was primarily due to diabetic macular edema.
Participants received faricimab (either every 2 months after 6 monthly loading doses or every 2, 3, or 4 months after 4 monthly loading doses) or aflibercept (every 2 months after 5 monthly loading doses).
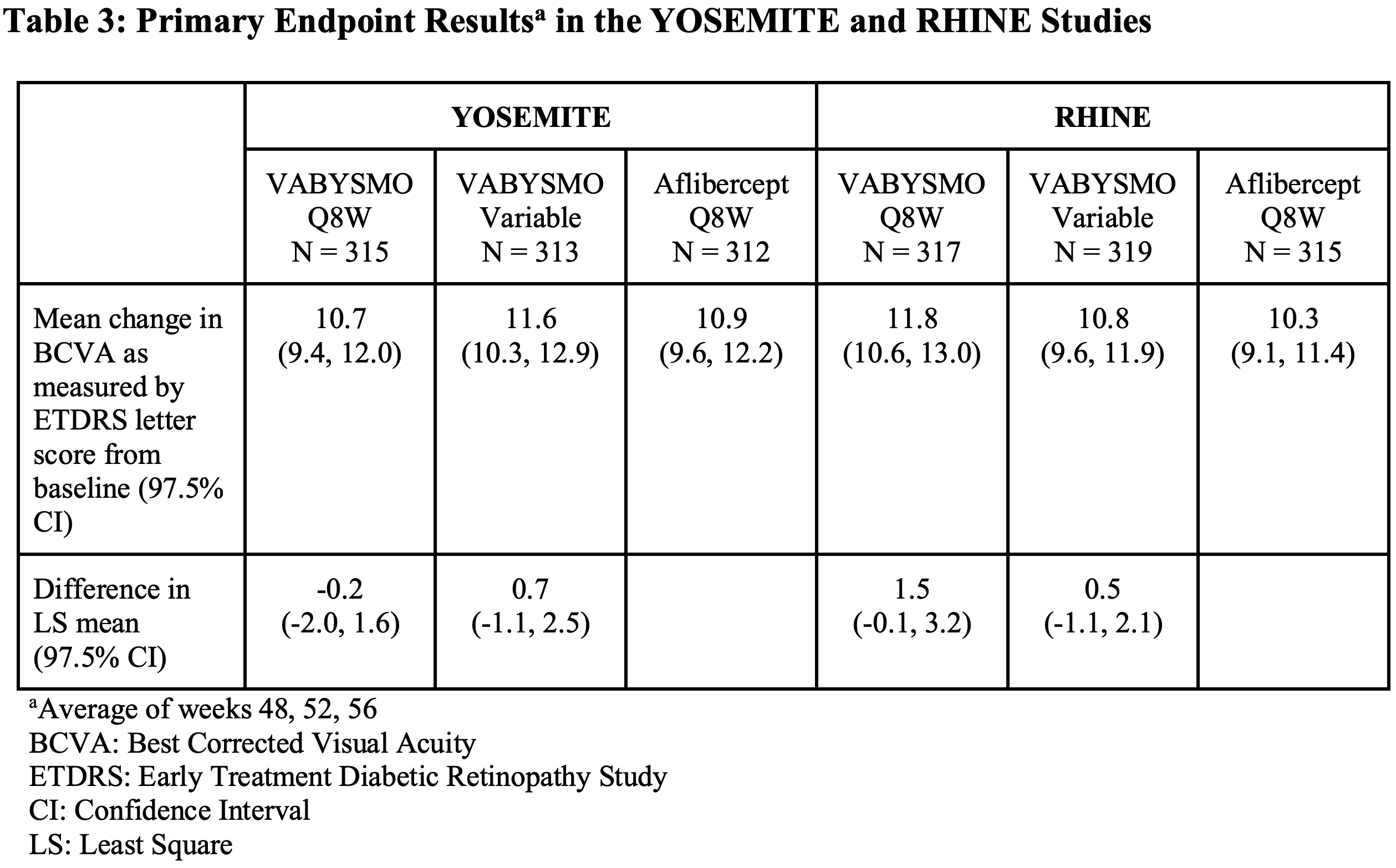
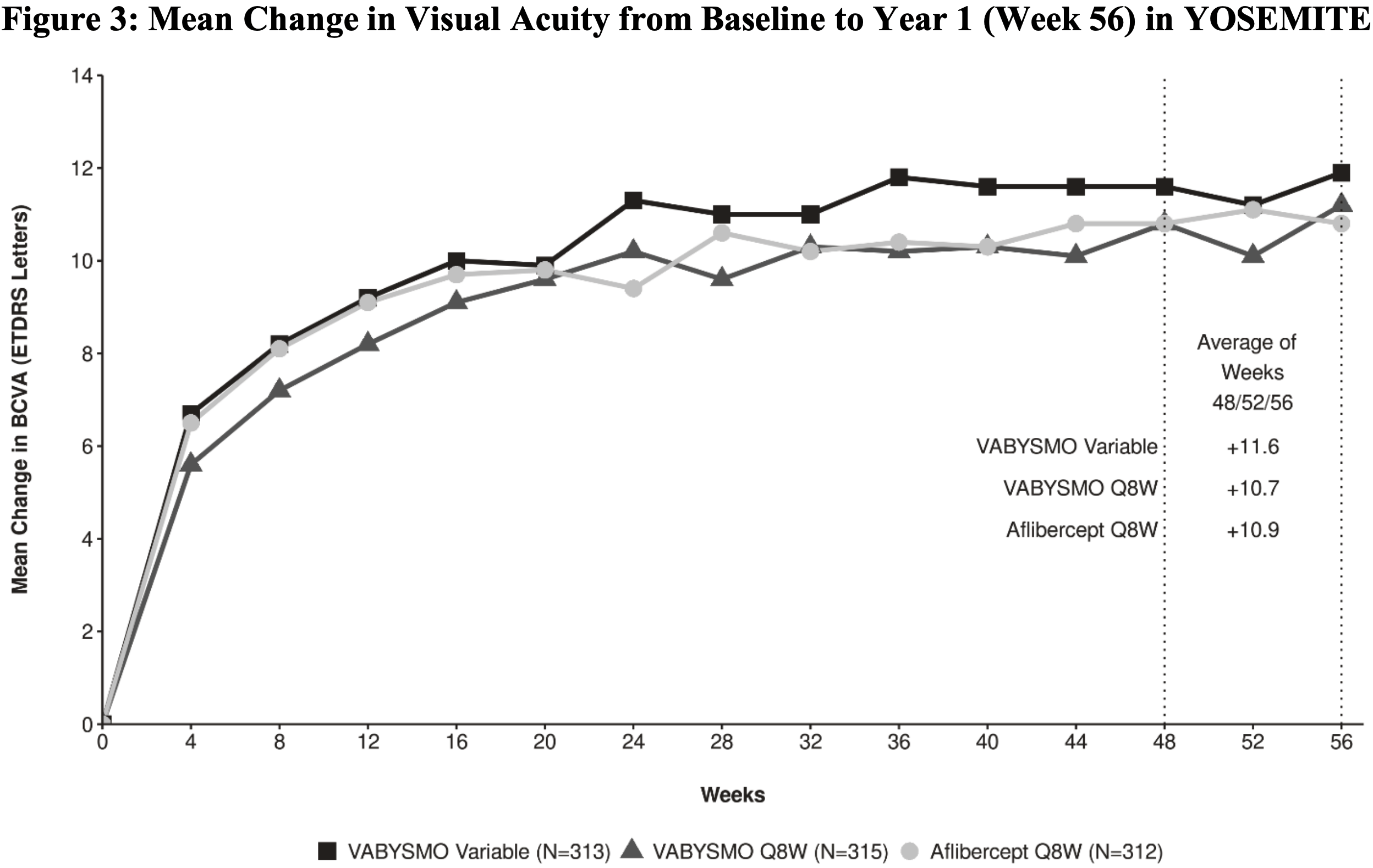
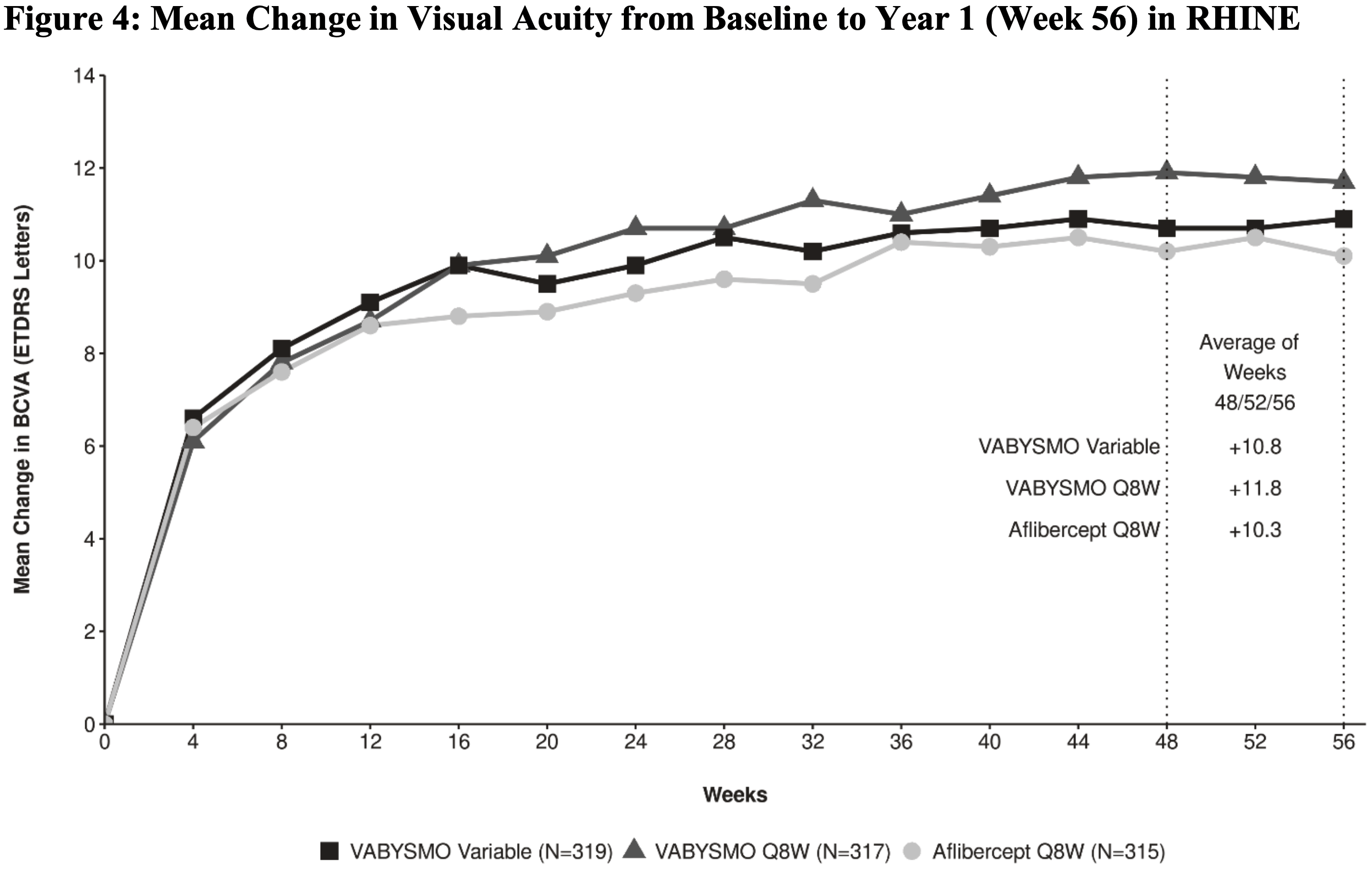
The primary endpoint of treatment efficacy was the change in Best-Corrected Visual Acuity (BCVA) averaged over 48, 52, and 56 weeks of therapy, according to the Early Treatment Diabetic Retinopathy Study (ETDRS) letter chart.
Vabysmo was found to perform as well as Eylea: in the fixed-dose faricimab, variable-dose faricimab, and aflibercept groups, respectively, the mean change in BCVA was 10.7 (97.5% CI: 9.4–12.0), 11.6 (97.5% CI: 10.3–12.9), and 10.9 (97.5% CI: 9.6–12.2) letters [in YOSEMITE], 11.8 (97.5% CI: 10.6–13.0), 10.8 (97.5% CI: 9.6–11.9), and 10.3 (97.5% CI: 9.1–11.4) letters [in RHINE].
Later, Roche disclosed the results of using Vabysmo for 2 years in the treatment of diabetic macular edema:
- Patients treated with Vabysmo demonstrated maintained visual improvement achieved after 1 year of treatment, and this improvement was non-inferior to that achieved with Eylea. The average visual gain in YOSEMITE was 10.7, 10.7, and 11.4 letters in the fixed-dose faricimab, variable-dose faricimab, and aflibercept groups, respectively, and 10.9, 10.1, and 9.4 letters in RHINE.
- Vabysmo provided improvement of at least 2 points, according to the Early Treatment Diabetic Retinopathy Study – Diabetic Retinopathy Severity Score (ETDRS-DRSS), in 42.8% and 44.3% of subjects in YOSEMITE and RHINE, respectively.
- Vabysmo did better than Eylea at reducing central subfield thickness (CST).
- Vabysmo was administered once every 4 months to 60% of patients in YOSEMITE and 64.5% in RHINE while maintaining a non-inferior performance of therapy compared with Eylea once every 2 months.
Vabysmo: Safety of Faricimab
The safety profile of Vabysmo, according to the frequency of adverse reactions, was generally not different from that of Eylea. Approximately equal proportions of patients experienced treatment-related adverse events such as conjunctival hemorrhage, vitreous floaters, retinal pigment epithelial tear, intraocular pressure increased, eye pain, intraocular inflammation (including iridocyclitis, iritis, uveitis, vitritis), eye irritation, ocular discomfort, vitreous hemorrhage.
Vabysmo: Expert Comments
Faricimab is a potential blockbuster: according to industry forecasts, Vabysmo could reach sales of $2.72 billion annually by 2026.
It should be understood, however, that faricimab has entered a riddled market of vascular endothelial growth factor (VEGF) inhibitors used in the treatment of wet age-related macular degeneration and diabetic macular edema. These drugs include Eylea (aflibercept) backed by Regeneron Pharmaceuticals and Bayer, Lucentis (ranibizumab) marketed by Roche and Novartis, and Beovu (brolucizumab) developed by Novartis. The anticancer Avastin (bevacizumab) by Roche is used off-label.
Vabysmo’s main competitor is Eylea, which earned $8.36 billion in 2020. Moreover, first, aflibercept will lose patent protection in the US and Europe in 2023 and 2025, thereby opening the door to less expensive biosimilars; second, Regeneron and Bayer are developing an 8-mg formulation of aflibercept (instead of 2-mg) for its use every 4 months.
Roche, aware of the intense competition, has set the cost of treating American patients at $2,190 per dose of Vabysmo (list price excluding discounts and rebates). And so the first year of treatment for wet age-related macular degeneration in a 4-month dosing cycle Vabysmo will cost $13,140, subsequent years of therapy will cost $6,570.
By comparison, the price of a single dose of Eylea is $1,940. The first year of treatment would cost $13,580, with subsequent years costing $11,640.
Meanwhile, Lucentis biosimilars have begun to appear, but Roche has prepared for this by offering a convenient replacement in the form of Susvimo (ranibizumab), an intraocular implant that is inserted once into the eye surgically in an outpatient setting and which is then refilled with the drug every six months.

Susvimo: Pioneering Implant for Treating Wet Age-Related Macular Degeneration
Roche offered a convenient replacement for the traditional Lucentis.
Outlook Therapeutics is preparing Lytenava (ONS-5010), an ophthalmic version of bevacizumab. For reference, the original Avastin is used off-label in half of all cases of wet age-related macular degeneration in the United States.
Australia’s Opthea is working on OPT-302, which blocks vascular endothelial growth factor C (VEGF-C) and vascular endothelial growth factor D (VEGF-D) and which, if given regulatory approval, will be administered together with aflibercept or ranibizumab.
Kodiak Sciences is developing KSI-301, an antibody biopolymer conjugate (ABC) against VEGF with an intravitreal dosing interval of up to 6 months.
Regenxbio has bet on RGX-314 (an anti-VEGF antibody fragment) gene therapy, a single application of which will permanently prevent VEGF-mediated formation of new leaky blood vessels and retinal fluid accumulation.
Switzerland’s Molecular Partners is trying to resolve questions about the safety of abicipar pegol (AGN-150998), which belongs to DARPins (designed ankyrin repeat proteins), which is targeted to VEGF-A and is administered once a quarter.
Extras
Vabysmo (faricimab). Prescribing information. U.S. [PDF]
Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022 Jan 21;S0140-6736(22)00010-1. [source]
Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022 Jan 21;S0140-6736(22)00018-6. [source]