Highlights
Talicia (omeprazole + amoxicillin + rifabutin, 10 mg/250 mg/12.5 mg) is a new combination drug indicated for primary eradication therapy of Helicobacter pylori infection in adults.
Talicia should be taken 4 capsules every 8 hours for 2 weeks.
Talicia offered by Israel’s RedHill Biopharma is approved by the U.S. Food and Drug Administration (FDA) in early November 2019.
The key ingredient in Talicia is rifabutin, which is the first new antibiotic approved to treat H. pylori infection in more than a decade.
Helicobacter pylori is a Gram-negative bacteria that is transmitted by the fecal-oral route and is present in the gastrointestinal (GI) tract of most half of humanity. H. pylori infection is a leading cause of upper GI diseases, such as chronic gastritis and peptic ulcer disease. It can lead to the development of gastric malignancies, including cancer and MALT lymphoma. H. pylori is also associated with dyspepsia, iron deficiency anemia, and vitamin B12 deficiency. [1] [2] [3] [4]
And if previously the eradication of H. pylori was successfully carried out with combination regimens that included antibiotics like clarithromycin, metronidazole, or levofloxacin, now — due to the increasing multidrug antibiotic resistance — treatment is often unsuccessful, forcing the transition to the next line of therapy.

Mechanism of Action of Talicia
In addition to the well-known proton pump inhibitor (PPI) omeprazole and the antibiotic amoxicillin, Talicia contains rifabutin, a broad-spectrum antibiotic.
Rifabutin is primarily a bactericidal antibiotic. Rifabutin, being a semi-synthetic derivative of rifamycin S, has a high affinity for prokaryotic RNA polymerase (and a very weak affinity for mammalian RNA polymerase), and therefore it easily binds to DNA-dependent RNA polymerase of bacteria, thus inhibiting their RNA synthesis.
Rifabutin has long been used in the treatment of tuberculosis and the prevention of infection of HIV patients with Mycobacterium avium bacteria. By the way, rifabutin is recommended for first-line therapy of tuberculosis, but rifampicin is widely prescribed due to its penny-pinching price. For HIV-positive people, rifabutin has the advantage over rifampicin of fewer drug interactions, making it more suitable for people on highly active antiretroviral therapy (HAART).
Talicia’s patent protection in the U.S. extends until 2034.
It might seem that to eradicate Helicobacter pylori it would be sufficient to turn to a generic version of rifabutin, but this is not the case. The bottom line is that sufficient intragastric exposure to antibiotics is critical to H. pylori eradication: If the proper concentration of the drug is lacking, therapy is unlikely to be successful. RedHill conducted a relevant study.
Thus, rifabutin administered in a dose of 50 mg every 8 hours provided its own intragastric concentration at or above the minimum inhibitory concentration, which suppresses the growth of 90% of bacteria (MIC90), for about 3 times longer than rifabutin taken in a dose of 150 mg once a day. Intragastric concentrations at or above MIC90 for approximately 93% over a 24-hour period were observed when rifabutin was taken with food in the first dosing option, compared to 35% for the second option.
This explains the low eradication rate of H. pylori (approximately 70%) when treated with generic versions of rifabutin (150-mg dose once daily). [1] [2]
Talicia: Effectiveness of Helicobacter pylori Eradication
The ERADICATE Hp2 (NCT03198507) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited adult patients (n=455) with previously untreated Helicobacter pylori infection whose diagnosis was confirmed by 13C-urease breath test (UBT) and gastric biopsy (from the gastric body and its antral region) for the presence of Campylobacter-like organism (CLO).
Participants were given either standard therapy (1000 mg amoxicillin, 40 mg omeprazole) or experimental treatment (1000 mg amoxicillin, 40 mg omeprazole, 50 mg rifabutin) every 8 hours for 2 weeks. Because rifabutin could cause chromaturia (changes in urine coloration), all subjects additionally received riboflavin to keep the blinding fair for the protocol.
The primary endpoint defined by a successful eradication of H. pylori (confirmed by negative UBT or stool antigen test results at least 28 days after completion of therapy) was reached by 83.8% of patients (95% CI: 78.4 to 88.0) in the Talicia therapy group — versus 57.7% of patients (95% CI: 51.2 to 64.0) in the standard therapy group. The difference between treatments was 26.1% (95% CI: 18.0 to 34.1) with a statistically significant difference in favor of Talicia (p<0.001).
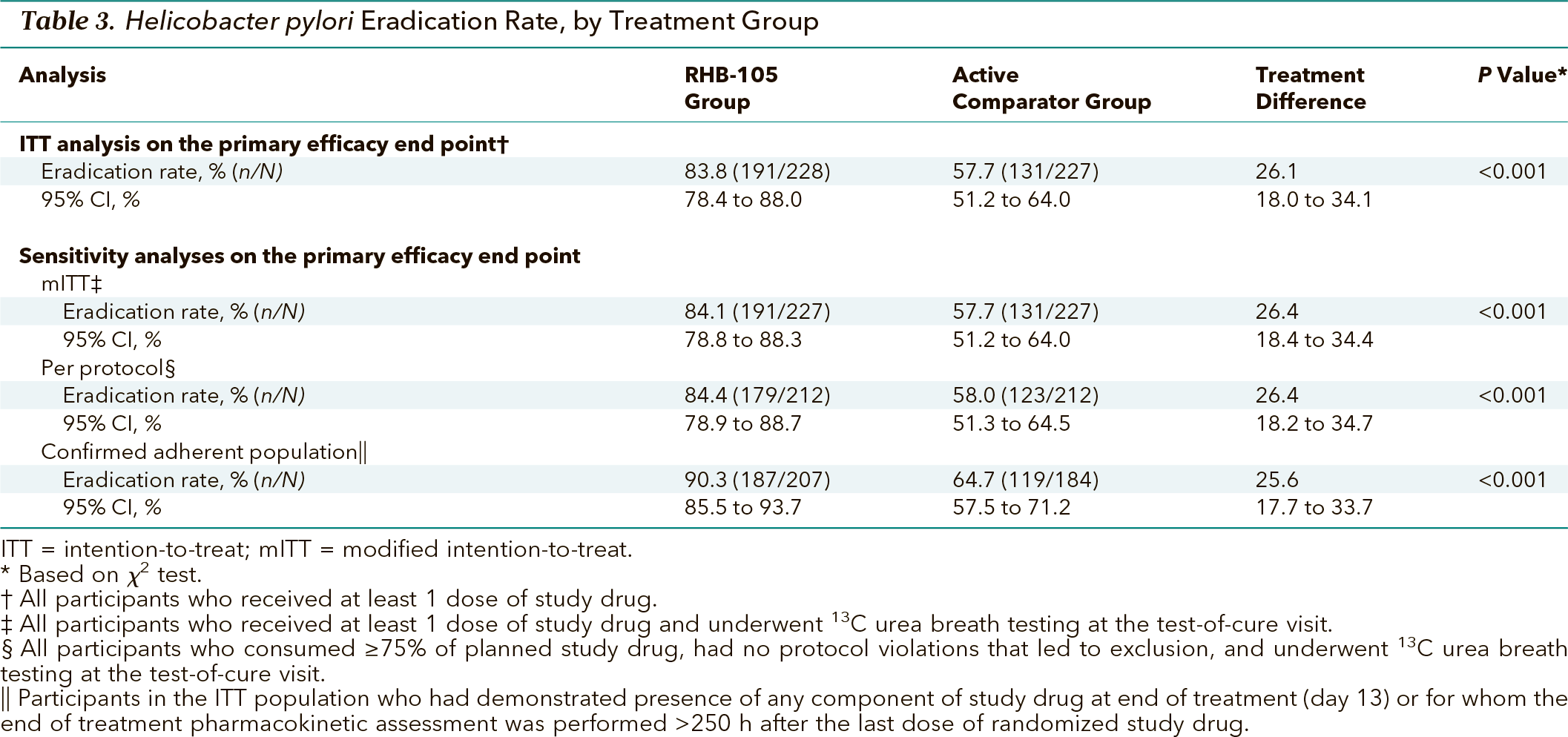
In a population of patients who strictly followed the course of treatment without skipping medication, the efficacy of getting rid of Helicobacter pylori in the Talicia group was 90.3% (95% CI: 85.5 to 93.7) — vs. 64.7% (95% CI: 57.5 to 71.2) in the control group: difference 25.6% (95% CI: 17.7 to 33.7); p<0.001.
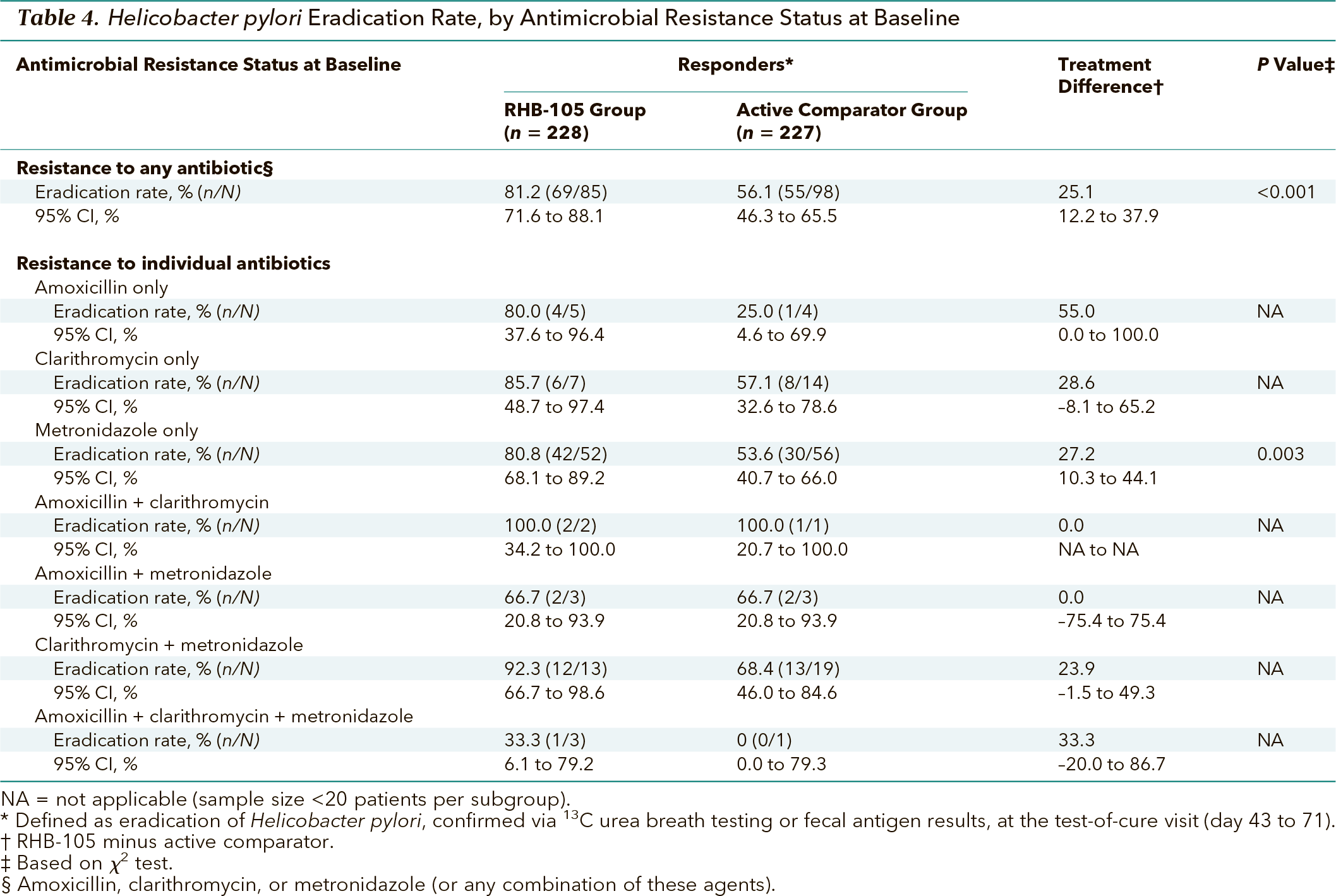
Talicia performed well in bypassing antibiotic resistance. Among patients with confirmed H. pylori resistance to prescription antibiotics such as amoxicillin, clarithromycin, metronidazole, or combinations thereof, the Talicia group demonstrated superiority over the standard Helicobacter pylori eradication group: a significantly higher proportion of subjects were free of it.
Talicia: Helicobacter pylori Eradication in Obesity
High body mass index (BMI) and obesity are known risk factors for failed Helicobacter pylori eradication. This is because excess adipose tissue alters drug deposition, affecting both the volume of distribution and clearance. This leads to insufficient minimum inhibitory concentration (MIC) of antibiotics, which is reflected not only in the failure of H. pylori eradication but also in the potential development of antibiotic resistance.
For example, while the rate of H. pylori eradication failure during triple clarithromycin therapy is 15% among patients with a BMI below 25 kg/m2, it is as much as 45% at higher BMIs.
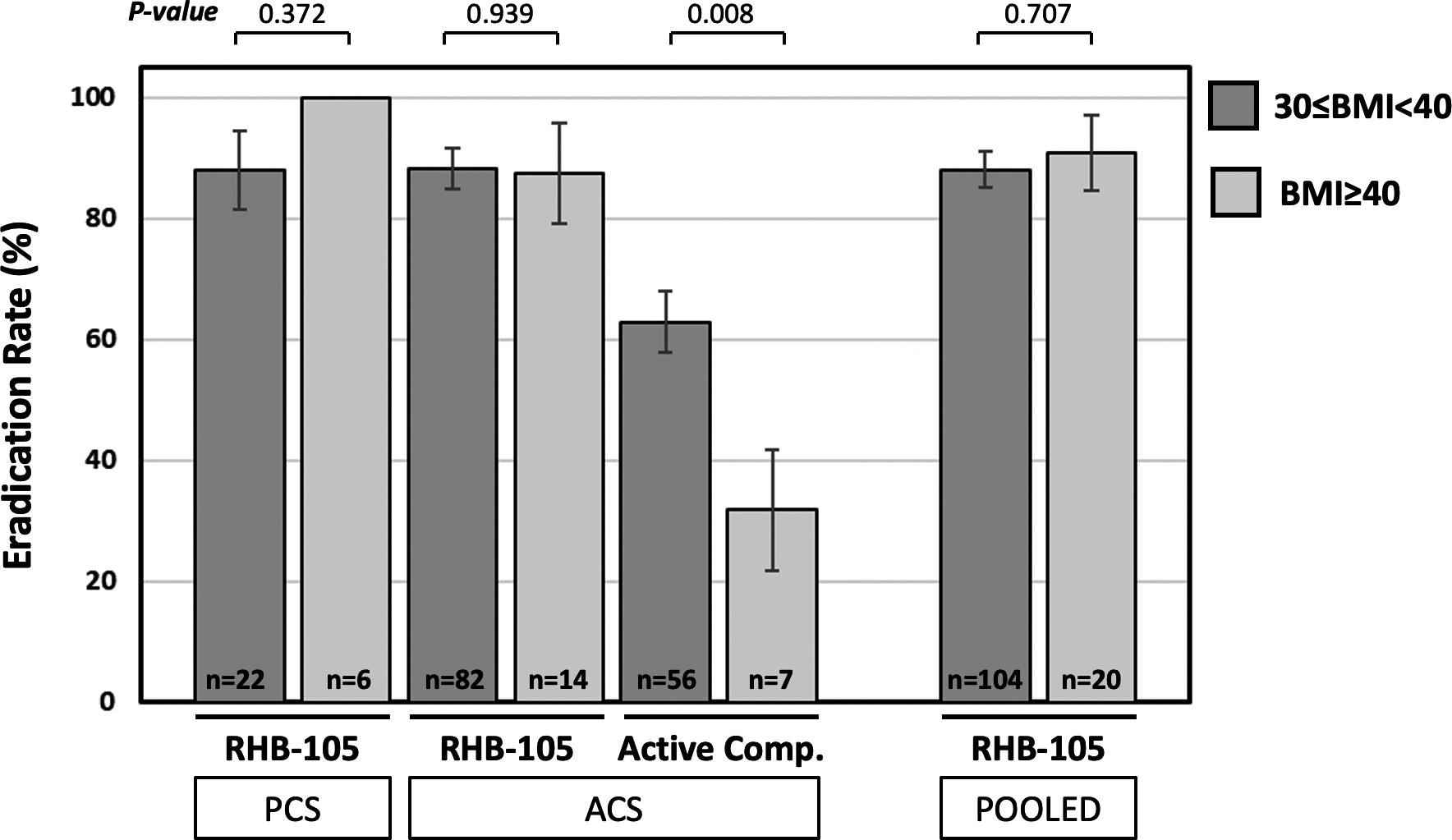
According to a retrospective analysis of data from subjects (n=269) collected in the ERADICATE Hp (NCT01980095) and ERADICATE Hp2 (NCT03198507) phase 3 clinical trials, treatment of obese patients with Talicia has demonstrated the highest level of effectiveness.
Thus, the rates of successful eradication of H. pylori among patients with BMI in the 30–40 kg/m2 and above 40 kg/m2 were 88.1% and 90.9%, respectively, in the Talicia groups — versus 62.9% and 31.8% in the comparison drug groups.
Given the prevalence of overweight and obesity everywhere, the unprecedented efficacy of Talicia should be taken as a gift from heaven.
Talicia and Helicobacter pylori Eradication: Systematic Review and Meta-analysis
A systematic review and meta-analysis of 33 prospective clinical trials (conducted up to the end of February 2020) that examined rifabutin for Helicobacter pylori eradication found a 73.2% (95% CI: 71.0 to 75.3) effectiveness of therapy with it (against proton pump inhibitor and amoxicillin) [I2=78.3, p<0.0001].
Three-component rifabutin-based therapy had an odds ratio (OR) of 1.40 (95% CI: 1.103 to 1.775) [I2=73.55, p=0.006] versus standard therapy.
Rifabutin administration was more clinically successful in the following cases:
- As part of first-line therapy versus rescue therapy (after failure of multiple lines): 82.4% (95% CI: 0.78 to 0.86, I2=27.44) success — vs. 71.3% (95% CI: 0.69 to 0.74, I2=79.35) [p=0.0001]
- Among the Asian population versus non-Asian one: 81.0% (95% CI: 0.74 to 0.86, I2=57.66) — vs. 72.4% (95% CI: 0.70 to 0.75, I2=80.41) [p=0.001]
- Augmented therapy (either daily doses of amoxicillin ≥ 3000 mg or proton pump inhibitor ≥ 80 mg or treatment duration of 14 days) versus less aggressive one: 80.6% (95% CI: 0.78 to 0.83, I2=71.19) — vs. 66.0% (95% CI: 0.63 to 0.69) [p=0.0001].
The incidence of adverse reactions in response to therapy with rifabutin was 25.3% (95% CI: 0.23 to 0.28) and the OR compared to the control group was 0.79 (95% CI: 0.57 to 1.09) [I2=61.58, p=0.15].
It should be understood that among the studies included in the meta-analysis, only one was a randomized, double-blind study that tested the first-line administration of rifabutin – all others were less reliable and valid. However, because of, first, the comparison of rifabutin with dual therapy (omeprazole and amoxicillin), which is not currently recommended as the first choice for successful eradication of H. pylori, and, second, its lack of comparison with four-component therapy (with or without bismuth), which is recommended for regions with high resistance to clarithromycin, it is not possible to unambiguously recommend rifabutin for first-line eradication of Helicobacter pylori.
Helicobacter pylori Eradication: Overview of Trends
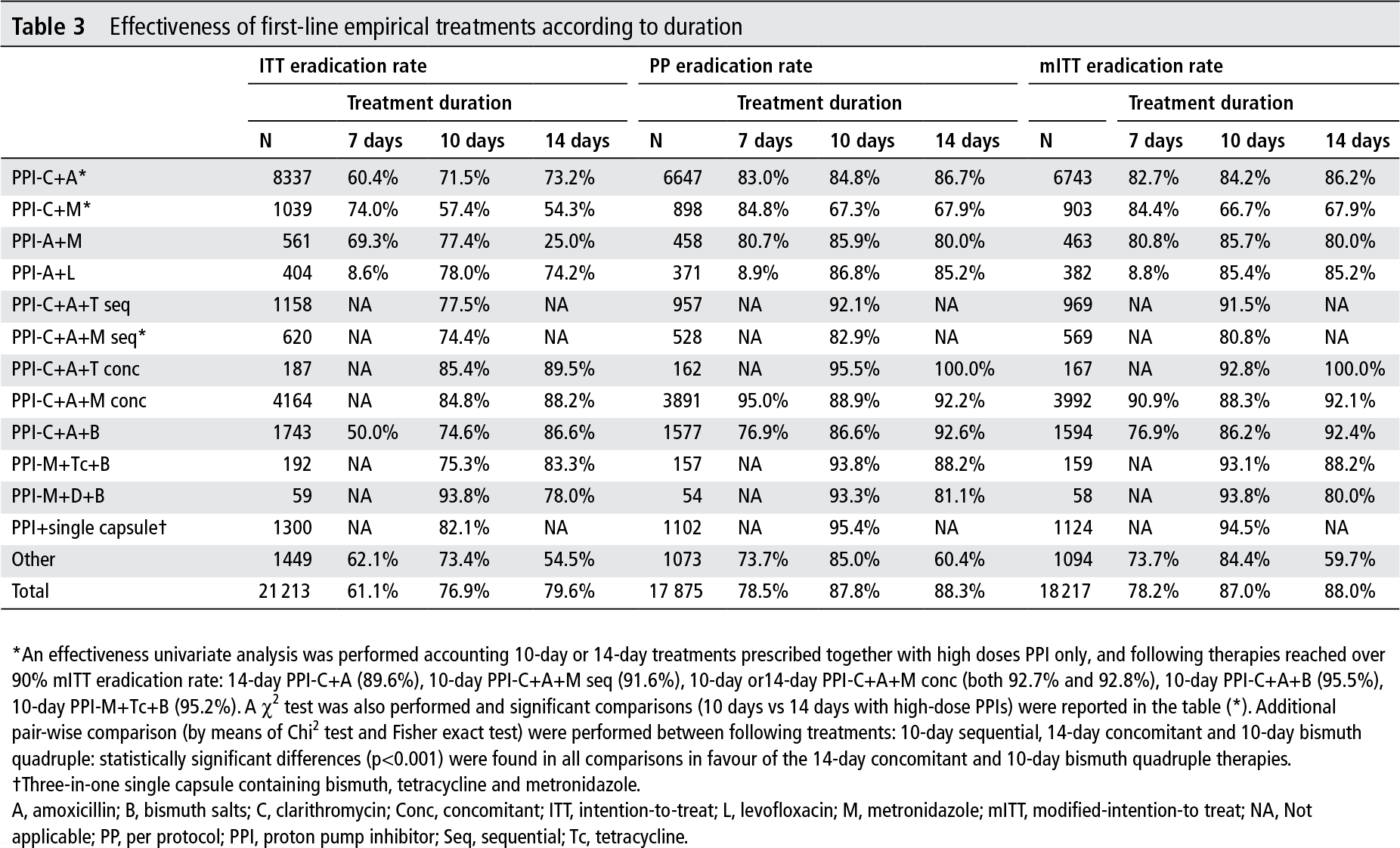
According to data from 21,500 patients from the European Helicobacter pylori infection treatment registry (Hp-EuReg) who underwent H. pylori eradication between 2013 and 2018, first-line empirical therapy was characterized by heterogeneity, suboptimality, and inconsistency based on treatment guidelines. It was noted that the chances of success increased with longer therapy, higher doses of proton pump inhibitor (PPI), and strict adherence to treatment.
Only 3 four-component treatment regimens achieved more than a 90 percent success rate of H. pylori eradication: PPI + amoxicillin + clarithromycin + metronidazole (tinidazole), 14 days; PPI + bismuth + amoxicillin + clarithromycin, 14 days; PPI + bismuth + tetracycline (doxycycline) + metronidazole, 10 days. If in a given geographic region there is a high level of antibiotic resistance (especially with dual resistance to clarithromycin and metronidazole over 15%), the latter bismuth-containing regimen is preferable.
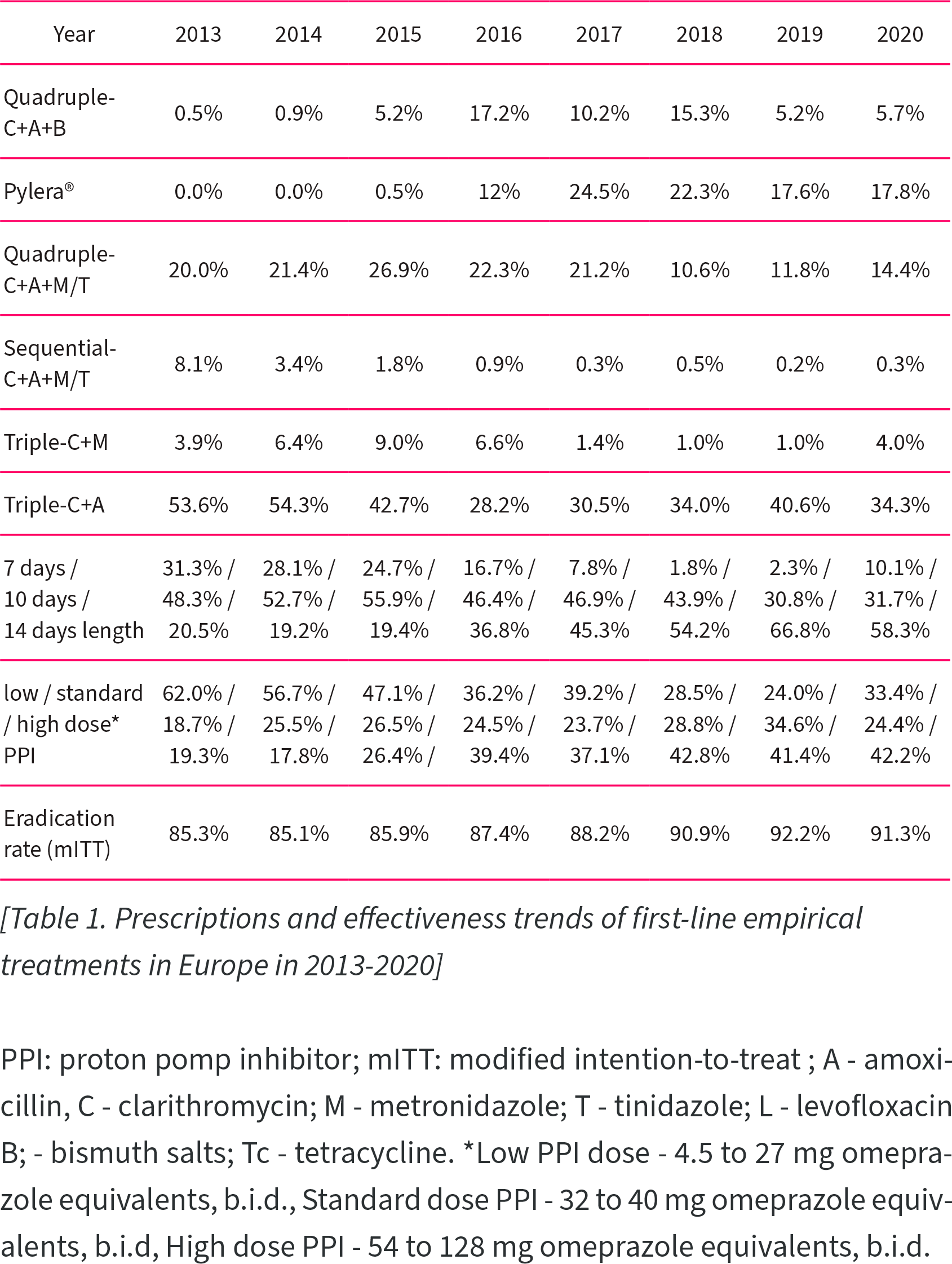
An updated analysis of data from 24,900 patients on Hp-EuReg registry for the period 2013–2020 documented that treatment efficacy of first-line empirical H. pylori eradication therapy increased from 85.3% to 91.3%.
Among the recorded trends: Decreasing popularity of three-component therapy, increasing interest in the single-capsule combination drug Pylera (bismuth + tetracycline + metronidazole), a longer course of treatment, increasing daily dose of PPI.
Extras
Talicia (omeprazole + amoxicillin + rifabutin). Prescribing information. U.S. [PDF]
Rifabutin-based triple therapy (RHB-105) for Helicobacter pylori eradication: A double-blind, randomized, controlled trial. Ann Intern Med. 2020 Jun 16;172(12):795-802. [source]
Rifabutin-containing triple therapy (RHB-105) for eradication of Helicobacter pylori: Randomized ERADICATE Hp trial. Antibiotics (Basel). 2020 Oct 9;9(10):685. [source]
Rifabutin triple therapy for first-line and rescue treatment of Helicobacter pylori infection: A systematic review and meta-analysis. J Gastroenterol Hepatol. 2020 Oct 10. [source]
Rifabutin for the treatment of Helicobacter pylori infection: A review. Pathogens. 2020 Dec 28;10(1):15. [source]
Helicobacter pylori eradication by low-dose rifabutin triple therapy (RHB-105) is unaffected by high body mass index. GastroHep. 2021 Sep 28. [source]
European Registry on Helicobacter pylori management (Hp-EuReg): Patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21 533 patients. Gut. 2021 Jan;70(1):40-54. [source]
Low-dose rifabutin triple therapy (RHB-105) demonstrates high Helicobacter pylori (H. pylori) eradication rates: Physiologically-based pharmacokinetic (PBPK) modeling supports favorable intragastric rifabutin concentrations for 50 mg Q8H dosing vs 150 mg QD. DDW 2022, May 21–24, 2022. [PDF]
Low-dose rifabutin triple therapy (RHB-105) maintains high Helicobacter pylori (H. pylori) eradication rates and shows favorable safety and efficacy in subjects with diabetes mellitus. DDW 2022, May 21–24, 2022. [PDF]