Highlights
In mid-December 2020, the experimental masitinib successfully passed a clinical trial in the therapy of patients with mild-to-moderate Alzheimer’s disease. On the wave of good news, the stock price of AB Science, the French company behind the development of masitinib, soared almost 70%.
Wall Street’s positive response is understandable: in view of the critical lack of drugs that would help with Alzheimer’s disease, even with a modicum of containment of the progression of cognitive deterioration. Many decades of searching for any drug that could alter the course of Alzheimer’s disease have turned out to be a failure in the form of several hundred flopped molecules.
The latest innovation for Alzheimer’s disease therapy is Oligomannate (sodium oligomannate), proposed by China’s Shanghai Green Valley Pharmaceuticals and made from brown algae. The idea was to modulate the gut microbiota in favor of getting rid of microglial-mediated neuroinflammation and amyloidosis.

Oligomannate: Finally New Drug to Treat Alzheimer’s Disease
Innovative Chinese medicine eliminates gut microbiota dysbiosis, and it helps slow the progression of dementia in Alzheimer’s disease.
A highly controversial one is aducanumab by Biogen, an experimental monoclonal antibody against amyloid beta, the accumulation of which in the brain is considered neurotoxic. A regulatory decision on aducanumab will be made by early June 2021.
By the way, AB is aptly positioned as a single-molecule pharmaceutical company; all of its activities are tied to the study of masitinib. The clinical validation program for masitinib is extensive. AB is trying to prove masitinib applicability in the therapy of amyotrophic lateral sclerosis, progressive forms of multiple sclerosis, severe asthma uncontrolled by corticosteroids, indolent systemic mastocytosis, and oncology diseases such as pancreatic cancer and prostate cancer.
Update #1
On June 1, 2021, AB notified that all clinical trials of masitinib have been suspended. The decision is related to the potential risk of ischemic heart disease with this experimental drug identified in a retrospective analysis of data from its clinical trials. Further information will be available once the safety profile of masitinib has been appropriately evaluated.
Update #2
At the end of August 2021, AB reported that the clinical trials of masitinib had resumed. At any rate, Norway has authorized continued enrollment of patients in phase 3 pivotal clinical trial AB19001 (NCT03127267) of masitinib for the treatment of amyotrophic lateral sclerosis. The study protocol includes all necessary interventions to prevent the risks of possible cardiac toxicity of masitinib.
Then, too, France allowed patients to be re-enrolled in phase 3 pivotal clinical trial AB15003 (NCT04333108) of masitinib for the treatment of mastocytosis.
In mid-September, the ban was lifted by the United Kingdom and the Netherlands, and Russia allowed phase 2 clinical trial AB20001 (NCT04622865) of masitinib in combination with isoquercetin for the treatment of moderate-to-severe COVID-19 infection in hospitalized patients.
In mid-November, the U.S. Food and Drug Administration (FDA) cleared further clinical study of masitinib in the treatment of amyotrophic lateral sclerosis.
Masitinib and Treatment of Alzheimer’s Disease: Efficacy and Safety
The clinical trial AB09004 (NCT01872598) phase 2b/3 (randomized, double-blind, placebo-controlled, multicenter, international) enrolled adult patients (n=718) with mild-to-moderate Alzheimer-type dementia; a total score on the Mini-Mental State Examination (MMSE) ranging from 12 to 25.
Subjects must have already been on at least a 6-month course of stable dose cholinesterase inhibitors (donepezil, rivastigmine, or galantamine) and/or memantine.
For 24 weeks, participants were given placebo twice daily or masitinib at a dose of 3.0, 4.5, or 6.0 mg/kg, on top of the aforementioned drugs.
Efficacy comparisons were made between the masitinib dose groups and separate placebo control groups for each of the drug doses.
The medium-dose masitinib group (n=182) showed statistically significant superiority over the placebo group (n=176):
- On the Alzheimer’s Disease Assessment Scale–Cognitive Subscale (ADAS-Cog), assessing patient’s cognitive ability and memory (word recall, following commands, orientation, praxis, etc.) [p=0.0003].
- On the Alzheimer’s Disease Cooperative Study–Activities of Daily Living (ADCS-ADL), assessing patient’s ability to independently perform routine activities and self-care (cooking, cleaning, walking, hygiene procedures, etc.) [p=0.0381].
In the low-dose masitinib group, a significantly lower proportion of patients experienced severe dementia (MMSE<10) [p=0.0446].
The safety profile of masitinib was characterized by tolerability. Adverse events were reported in 87.0% of patients treated with masitinib — versus 77.5% in the control group. Serious ones were reported in 13.0% and 5.4%, and severe ones in 26.5% and 19.3%, respectively.
Masitinib and Alzheimer’s Disease Treatment: Detailed Results of Therapy Effectiveness
On the ADAS-Cog scale, according to an analysis of covariance (ANCOVA), the least squares mean (LSM; henceforward) change in the 4.5-mg/kg masitinib dose group was −1.46 points (95% CI: −2.46 to −0.45) — versus +0.69 points (95% CI: −0.36 to +1.75) in the control group. The difference was −2.15 points (97.5% CI: −3.48 to −0.81) [p=0.0003].

It should be understood that for the primary analysis with the full set of patients, a missing data imputation model was applied: previous validated patient assessment and data from similar patients (from the same cluster) who were continuing therapy were used instead.
Nevertheless, the statistical significance of masitibine persisted in the primary analysis with the most conservative approach (Jump to Reference, J2R), in which missing data from all patients who prematurely discontinued treatment (due to lack of efficacy or toxicity) were imputed by placebo data. The change was −1.04 points (95% CI: −2.06 to −0.03) — vs. +0.85 points (95% CI: −0.21 to +1.91). The difference came out to −1.89 points (95% CI: −3.06 to −0.72) [p=0.0016].

On the ADCS-ADL scale, according to the ANCOVA model with missing data imputation, the change was +1.01 points (95% CI: −0.48 to +2.50) — vs. −0.81 points (95% CI: −2.36 to +0.74). The difference was +1.82 points (97.5% CI: −0.15 to +3.79) [p=0.0381].

On the strict J2R approach, the masitinib group showed a numerical superiority over the control group that was close to statistically significant: the LSM change was +0.81 points (95% CI: −0.68 to +2.30) — vs. −0.90 points (95% CI: −2.46 to +0.65). The difference came out to +1.71 points (95% CI: −0.01 to +3.43) [p=0.0512].

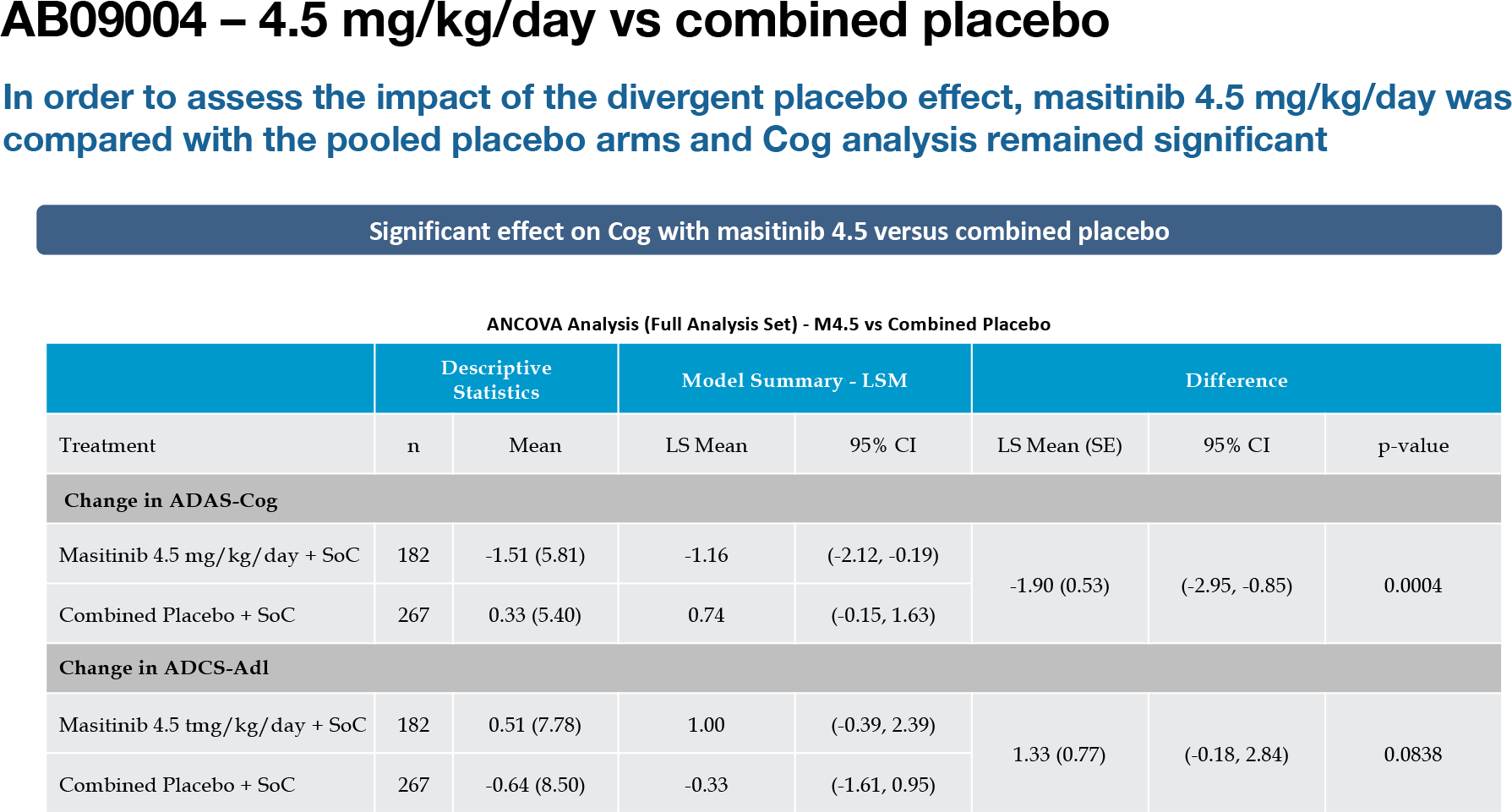
AB also performed a post hoc analysis (ANCOVA) of the data in a modified population that excluded some patients (who did not comply with or adhere to treatment appropriately) and included those previously discarded (for a variety of reasons). It turned out that masitinib retained statistical significance on the ADAS-Cog scale (p=0.0004) but lost it on the ADCS-ADL scale (p=0.07426).

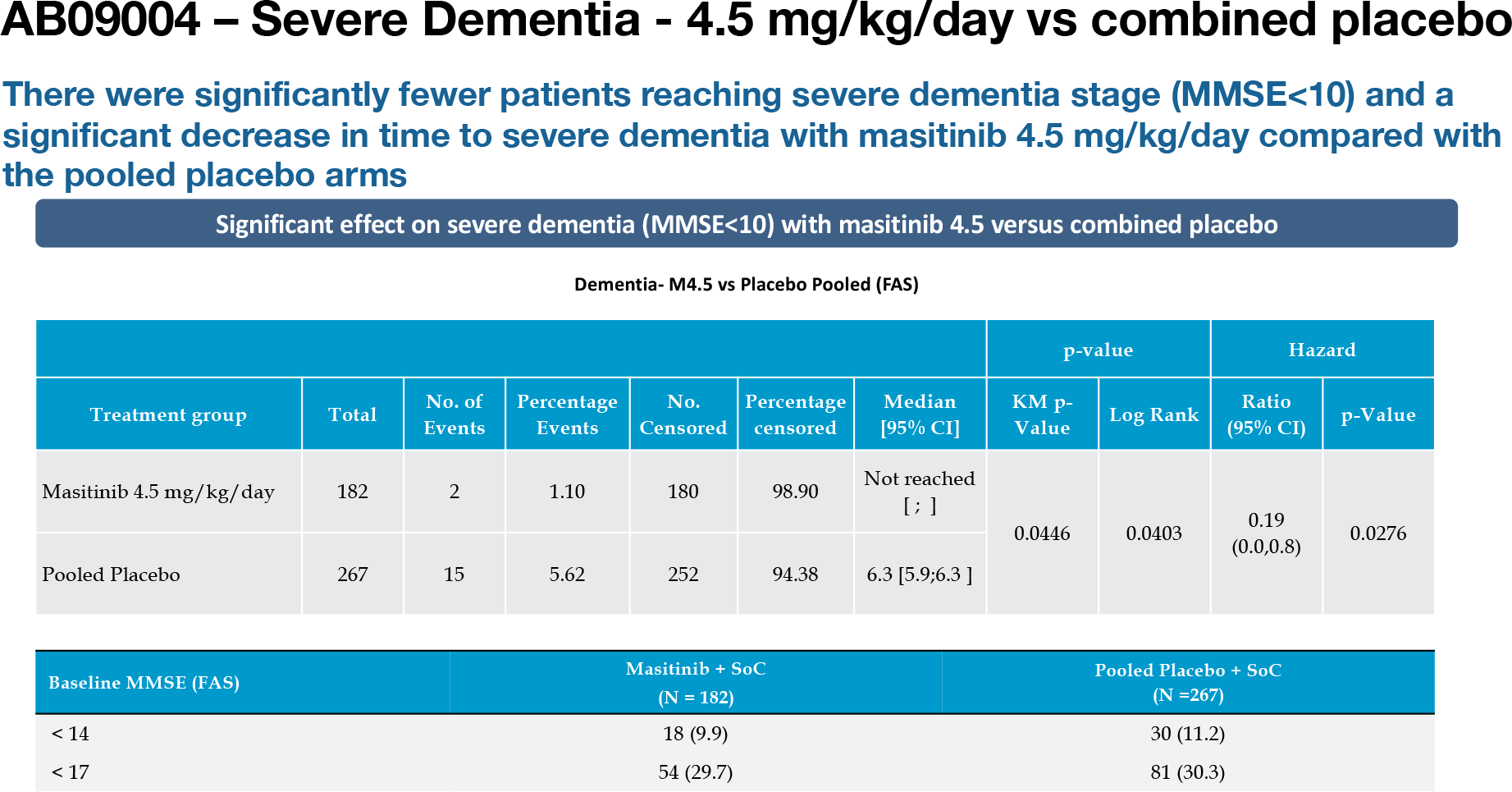
The 4.5-mg/kg masitinib group was compared to the pool of outcomes in all placebo groups (n=267), not just the placebo group corresponding to this dose of drug (n=176), in order to assess the impact of the divergent placebo effect. The statistical significance of masitinib on the ADAS-Cog scale (p=0.0004) but not on the ADCS-ADL scale (p=0.0838) was confirmed. Masitinib was able to delay the time to the development of severe dementia (p=0.0276).
Administration of masitinib resulted in a statistically significant change in the Clinician’s Interview–Based Impression of Change with caregiver’s input (CIBIC+) score: a 71% improvement (p=0.0400).

The masitinib group showed numerical superiority over the placebo group in scores on the Mini-Mental State Examination (MMSE), the Clinical Dementia Rating (CDR), and the Neuropsychiatric Inventory (NPI).

Masitinib in Alzheimer’s Disease: Mechanism of Action
There are three things whose role in the pathogenesis of Alzheimer’s disease is underestimated: the blood-brain barrier (BBB) [1], neuroinflammation [2], and mast cells. And they are closely related to each other.
Mast cells are located on both sides of the BBB and can rapidly cross it, building up their own population in response to a number of stimuli [3][4][5]. Mast cells play an important role in maintaining the inflammatory network of the central nervous system [6], including through the release of large amounts of proinflammatory mediators and the ability to modulate the permeability of the BBB [7]. All this has therapeutic implications, since a defective BBB is quite common in neuroinflammatory and neurodegenerative diseases such as Alzheimer’s disease.
Alzheimer’s disease is associated with pathological neurotoxic aggregation of amyloid beta plaques and tau-positive neurofibrillary tangles. Mast cells are activated by various stimuli, including amyloid beta peptides [8]. This leads to increased permeability of the BBB and increased accumulation of amyloid beta in the brain.
Oral masitinib (AB1010) is a small-molecule selective inhibitor of receptor tyrosine kinases (RTKs) class III; those belonging to the platelet-derived growth factor receptor (PDGFR) family. Masitinib, primarily targeted against the c-Kit proto-oncogene, also shows activity against PDGFR, lymphocyte-specific protein tyrosine kinase (Lck), colony stimulating factor 1 receptor (CSF1R, FMS), Fyn-related kinase (FRK, PTK5), LYN proto-oncogene, discoidin domain receptor tyrosine kinase 2 (DDR2, CD167b).
By the way, according to the Gini coefficient, masitinib is one of the most highly selective kinase inhibitors. In other words, this allows hoping for an improved safety profile among drugs related to tyrosine kinase inhibitors.
The mechanism of action of masitinib in Alzheimer’s disease is explained as follows. First, masitinib, co-targeting against c-Kit and Lyn, controls mast cell survival, differentiation, and degranulation, thereby indirectly regulating an array of pro-inflammatory and vasoactive mediators. This results in restoration of the integrity of the BBB and leads to inhibition of neuroinflammation by blocking the entry of amyloid beta peptides and pro-inflammatory mediators into the brain.
Second, masitinib inhibits Fyn activity involved in Alzheimer’s disease pathogenesis because it participates in amyloid beta signaling and tau protein phosphorylation. In addition to blocking amyloid and tau protein neurotoxicity, this results in inhibition of neuronal injury due to overactivation of the N-methyl-D-aspartate receptor (NMDAR) and synaptic death.
Thus, by preventing neuroinflammation and dendritic spike defects in patients with Alzheimer’s disease, masitinib can improve synaptic plasticity and dendritic integrity in memory circuits without directly affecting amyloid pathology.
An additional study concluded that blocking hemichannels on mast cells and glial cells by masitinib to inhibit the release of cytokines and other bioactive proinflammatory substances is a promising new strategy to combat the progression of neurodegenerative diseases.
Masitinib for Alzheimer’s Disease: What’s Next
What remains unclear is the issue with the high-dose masitinib group, which received it twice daily at a dose of 4.5 mg/kg for 3 months and then, for the next 3 months, at 6 mg/kg. Theoretically, this should have been mirrored by an increase in the therapeutic efficacy of masitinib. However, the higher dose did not result in a statistically significant increase in treatment efficacy (when compared with the 4.5-mg/kg dose), although it did not exhibit more severe adverse reactions mediated by inhibition of platelet-derived growth factor (PDGF) which is involved in maintaining certain cellular phenotypes in the central nervous system.
AB is about to launch a pivotal clinical trial of masitinib in the treatment of Alzheimer’s disease. The results of the study, which will also include patients from the U.S. and Europe, are expected to be collected by 2023.
It is claimed that the patent protection of masitinib will last until 2028 (composition and synthesis) and until 2041 (method of use in Alzheimer’s disease therapy).
One More Thing
AB’s current commercial activity is primarily in the marketing of masitinib for veterinary medicine. The drug, approved in Europe in November 2008 as Masivet (masitinib), is used in the treatment of nonresectable mast cell tumors (with confirmed mutated tyrosine kinase receptor c-Kit) in dogs.

In December 2015, veterinary Kinavet (masitinib) lost its U.S. registration, where it had been conditionally approved in December 2010 for the treatment of recurrent (post-surgery) or nonresectable cutaneous mast cell tumors in dogs: AB did not provide clinical data within five years that would conclusively confirm the drug’s efficacy.
If masitinib does get approved for human therapy, it will probably get the following brand names: Alsitek, Masiviera, Masipro, or Masican.
Extras
AB Science. Corporate presentation, October 2021. [PDF]
Masitinib in Alzheimer’s disease. AB Science. 11 December, 2020. [PDF]
Masitinib as an adjunct therapy for mild-to-moderate Alzheimer’s disease: a randomised, placebo-controlled phase 2 trial. Alzheimers Res Ther. 2011 Apr 19;3(2):16. [source]
Masitinib for the treatment of mild to moderate Alzheimer’s disease. Expert Rev Neurother. 2015 Jun;15(6):587-96. [source]
Effects of chronic masitinib treatment in APPswe/PSEN1dE9 transgenic mice modeling Alzheimer’s disease. J Alzheimers Dis. 2020;76(4):1339-1345. [source]
Masivet (masitinib). Veterinary prescribing information. Europe. [PDF]
Kinavet (masitinib). Veterinary prescribing information. US. [PDF]
Masitinib: scientific data for veterinary medicine. [PDF]
Masitinib: the efficacy of targeted therapy in veterinary medicine. [PDF]