Highlights
Prevnar 20 is a new vaccine indicated for active immunization adults to prevent pneumonia and invasive pneumococcal disease caused by Streptococcus pneumoniae.
Prevnar 20, developed by Pfizer, is approved by the U.S. Food and Drug Administration (FDA) in June 2021.
The European Medicines Agency (EMA), which accepted Prevnar 20’s application in late February 2021, continues to review it.
Prevnar 20 protects against the main cause of bacterial pneumonia, S. pneumoniae, with twenty different serotypes: 1, 3, 4, 5, 6A, 6B, 7F, 8, 9V, 10A, 11A, 12F, 14, 15B, 18C, 19A, 19F, 22F, 23F, 33F. However, regulatory approval for protection against serotypes 8, 10A, 11A, 12F, 15B, 22F and 33F has been granted on an accelerated basis, meaning that for these pneumococcal serotypes the vaccine has yet to definitively prove its own preventive efficacy.
Prevnar 20 is a further development of the 13-valent Prevnar 13 vaccine, which has made billions of dollars for Pfizer. Prevnar 20 added to Prevnar 13 protection against the aforementioned seven serotypes of S. pneumoniae, which are associated with high rates of mortality, antibiotic resistance, and meningitis.
Prevnar 20 Pneumococcal Vaccine: Effectiveness of Protection Against Pneumonia
The prophylactic efficacy of Prevnar 20, first, builds on the clinical validation of the predecessor Prevnar 13 vaccine and, second, has been established in three separate clinical trials.
Thus, the CAPiTA (NCT00744263) phase 4 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled Netherlands resident volunteers (n=84496) aged 65 years or older who were administered a single dose of Prevnar 13 or placebo.
The primary endpoint was the prophylactic efficacy of Prevnar 13 in the task of preventing the first episode of vaccine-type pneumococcal community-acquired pneumonia (VT-CAP), as confirmed by the presence of at least two clinical criteria and chest X-ray, and a positive VT-specific urinary antigen detection assay or isolation of vaccine-type S. pneumoniae from blood or another sterile site.
Among the secondary endpoints: prevention of the first episode of confirmed nonbacteremic and noninvasive VT-CAP (blood culture and any other sterile site results are negative for S. pneumoniae) and the first episode of confirmed invasive pneumococcal disease (with the presence of S. pneumoniae in sterile sites).
After nearly 4 years of follow-up, the group of subjects who received Prevnar 13 statistically significantly outperformed the placebo group in the task of preventing the first episode of infection caused by S. pneumoniae serotypes included in this vaccine.
Thus, community-acquired pneumonia developed in 49 people in the vaccine group — versus 90 in the placebo group: Prevnar 13 efficacy was 45.6% (95.2% CI: 21.8–62.5).
Nonbacterial and noninvasive community-acquired pneumonia occurred in 33 subjects — vs. 60: Prevnar 13 efficacy came out to 45.0% (95.2% CI: 14.2–65.3).
The invasive pneumococcal disease occurred in 7 — vs. 28 participants: efficacy of Prevnar 13 was 75.0% (95.2% CI: 41.4–90.8).

Three phase 3 clinical trials evaluated the safety and immunogenicity of Prevnar 20 among more than 6,000 adult participants (including adults aged 65 and older), both previously unvaccinated for pneumonia and those who had done so:
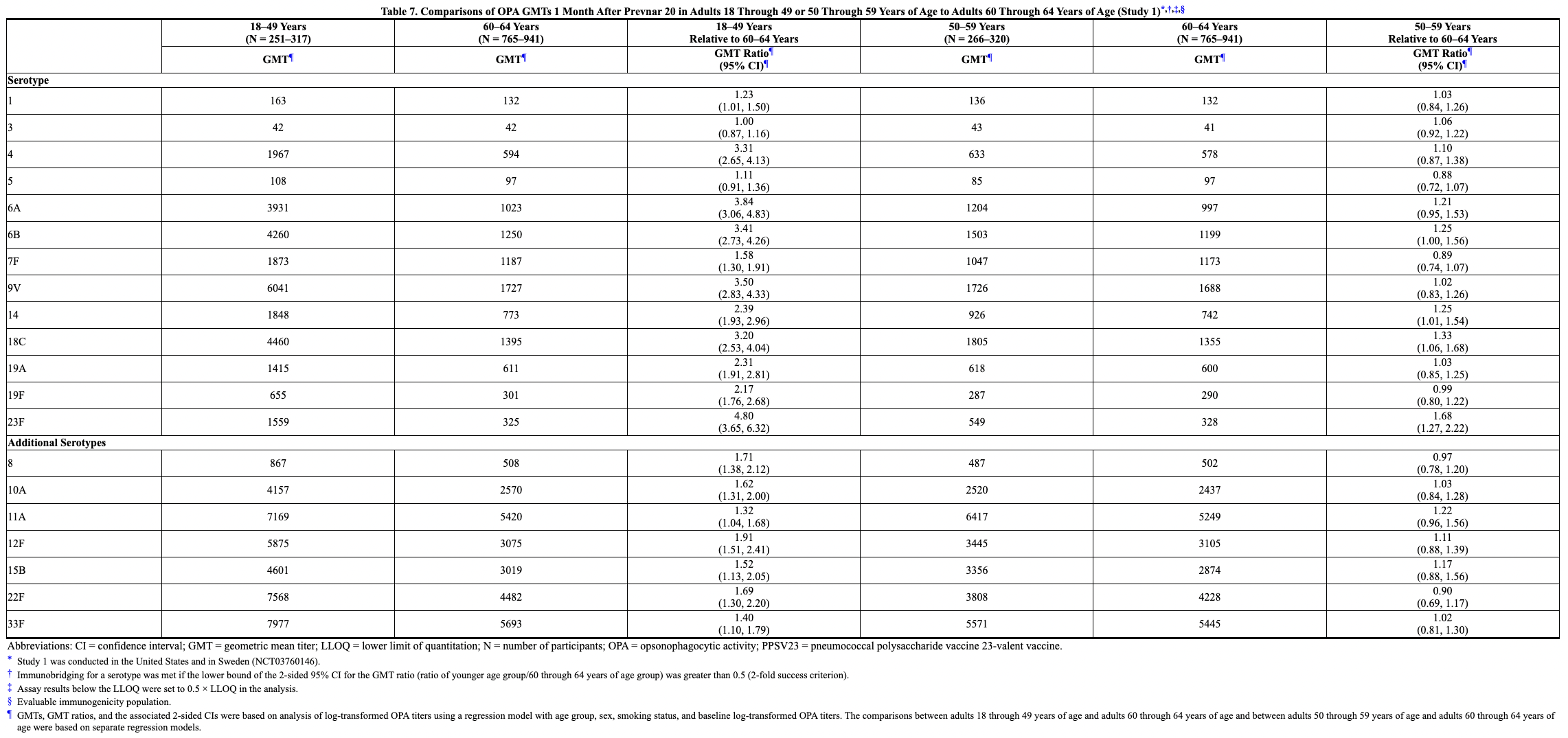
- NCT03760146: previously unvaccinated for pneumonia — comparing immune responses among people age 60 or older after Prevnar 20, Pneumovax 23 by Merck & Co., or placebo vaccination, and evaluating immune responses to Prevnar 20 versus Prevnar 13 among participants aged 18–59 years;
- NCT03828617: previously unvaccinated for pneumonia — comparing immune responses among people aged 18–49 years after Prevnar 20 or Prevnar 13 vaccination;
- NCT03835975: previously vaccinated for pneumonia — comparing immune responses among subjects age 65 or older after Prevnar 20, Prevnar 13, or Pneumovax 23 vaccination.
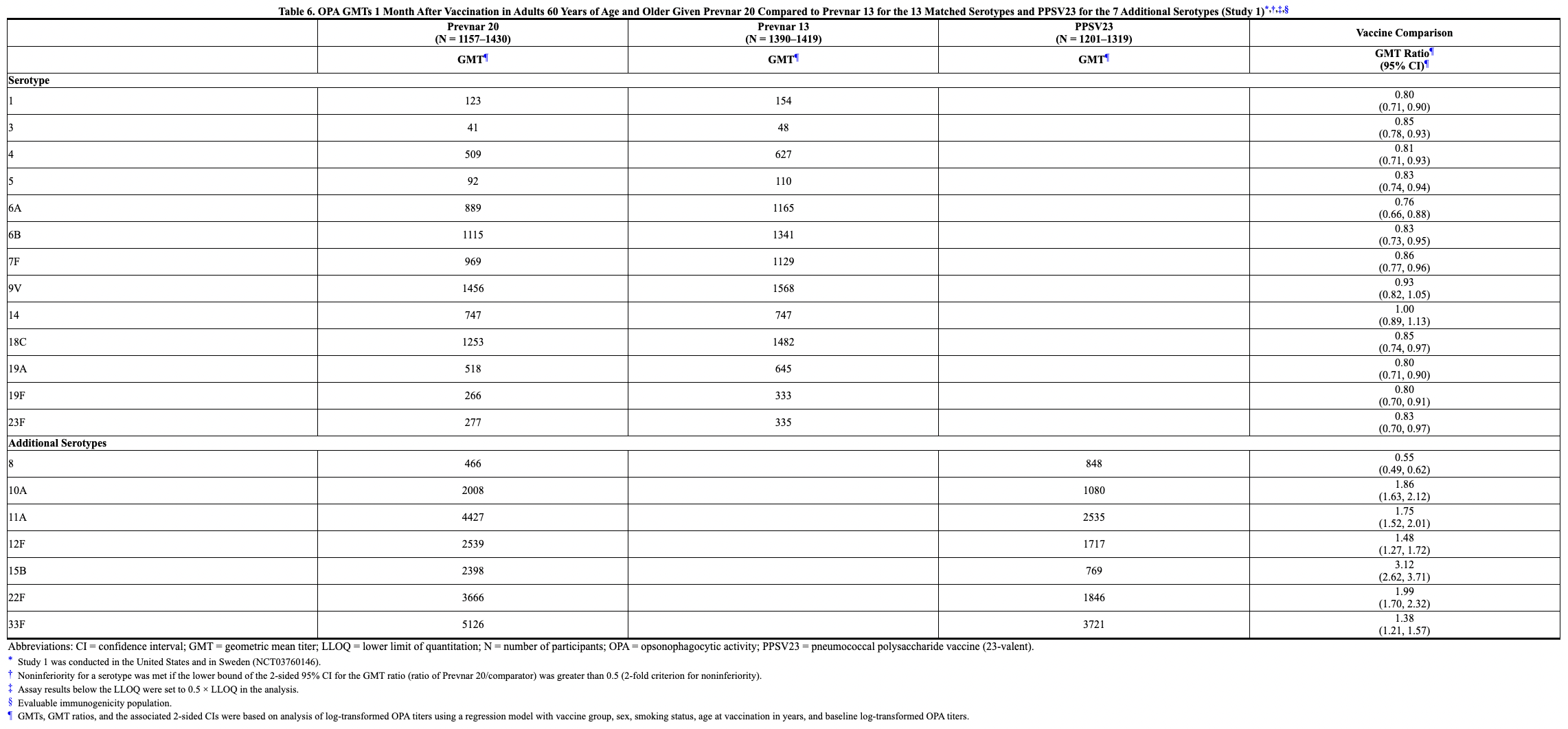
Immune responses generated by Prevnar 20 were found to be not inferior to those in the control groups, according to an opsonophagocytic activity assay measuring the titer of functional serotype-specific antibodies to S. pneumoniae 1 month after vaccination. The titer of opsonic antibodies predicting protection against invasive pneumococcal disease or pneumococcal pneumonia was not measured.
Prevnar 20 Pneumococcal Vaccine: How It Works
Streptococcus pneumoniae is the leading cause of community-acquired pneumonia, responsible for more than 2 million deaths per year, especially among children, the elderly, and those with compromised immune systems. The disease usually occurs without bacteremia (without the presence of bacteria in the blood), although a quarter of cases develop the invasive pneumococcal disease, characterized by infection of usually sterile sites.
Immunological protection from pneumococcal infection is provided by opsonophagocytic antibodies against the capsular polysaccharides of S. pneumoniae, which determine the serotypes of this bacteria and serve as virulence factors. Vaccines consisting of purified capsular polysaccharides became available over 50 years ago. The 23-valent Pneumovax 23, the first such pneumonia vaccine, was offered in 1983.
The protective efficacy of vaccines can be enhanced by conjugating the bacterial polysaccharide with an immunogenic carrier protein. In the case of Prevnar 20 (as well as Prevnar 13), each of the 20 pre-purified S. pneumoniae capsule antigens is chemically activated and linked to diphtheria anatoxin CRM197 (this protein is highly immunogenic but not toxic) to form a glycoconjugate, which in turn undergoes a purification procedure. After the introduction of Prevnar 20, the immune system begins to produce functional antibodies that implement the opsonophagocytic destruction of S. pneumoniae upon infection.
Such a combination induces a much stronger immune response (compared to Pneumovax 23) and does so by recruiting CRM197-specific type 2 T helpers, which switches the immunoglobulin type (in order to produce non-IgM immunoglobulins) and organizes memory B cells synthesis. Mucosal immunity also develops and eventually lifelong immunity after several exposures.
Prevnar 20 Pneumococcal Vaccine: Competitive Environment
Merck & Co.
Prevnar 20 (PF-06482077, 20vPnC), a pneumococcal 20-valent conjugated polysaccharide vaccine, is considered more effective than Pneumovax 23 by Merck & Co. which, although offering prevention of 23 Streptococcus pneumoniae serotypes, is made with traditional and less effective polysaccharide technology, not backed by an immunogenic carrier protein.
- For reference: Pneumovax 23 adds protection against serotypes 2, 9N, 17F, and 20, but lacks protection for 6A. Pneumovax 23 is ineffective in protecting children younger than 2 years of age because of the immaturity of their immune system. It does not always work in the elderly.
It is important for Pfizer to strengthen its position in the pneumococcal vaccine sector. First, Merck & Co. is stepping on its heels with a 15-valent conjugated polysaccharide vaccine, Vaxneuvance (V114), approved by the FDA in July 2021.

Astellas Pharma and Affinivax
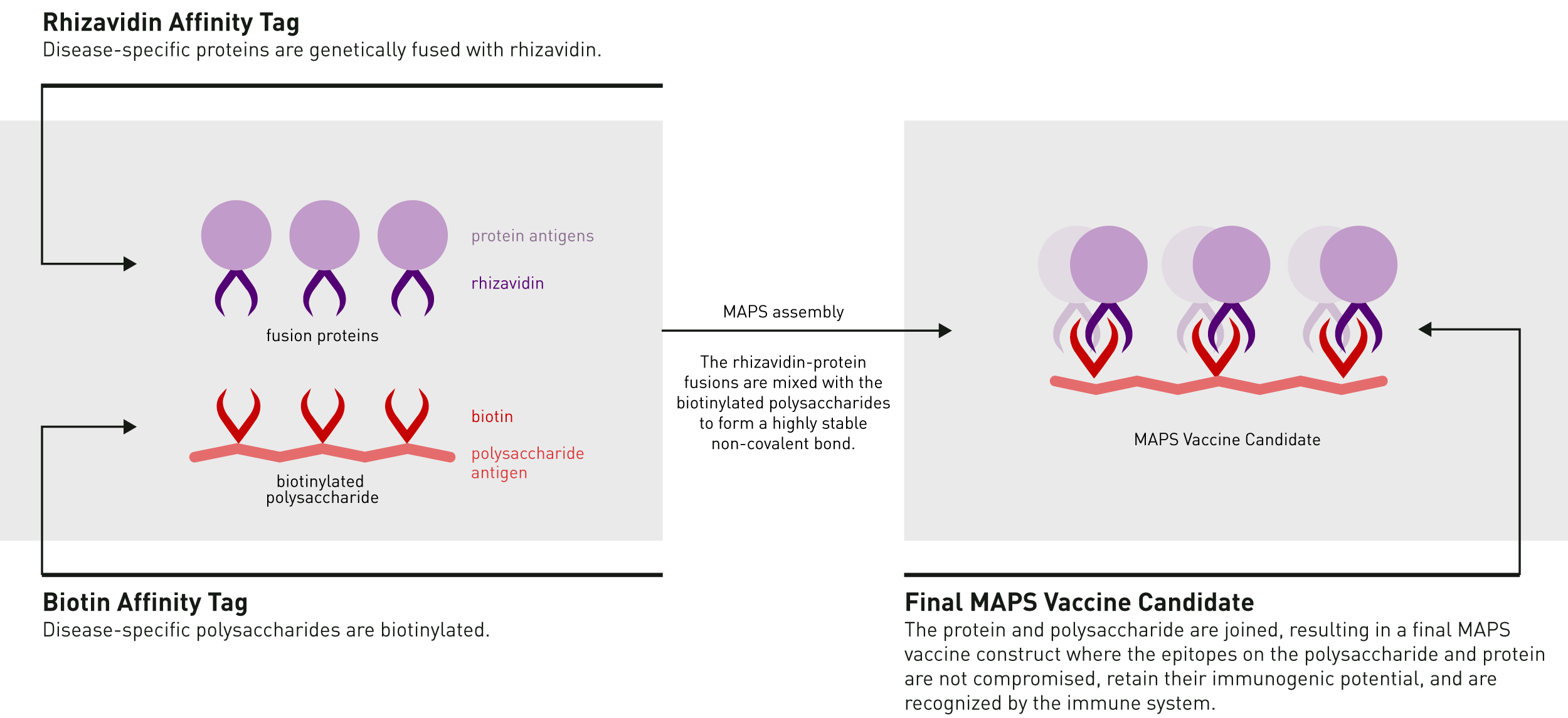
Second, more advanced pneumococcal vaccines are coming. For example, Astellas Pharma and Affinivax are working on Multiple Antigen Presenting System (MAPS) platform to create highly effective vaccines with the broadest coverage of serotypes.
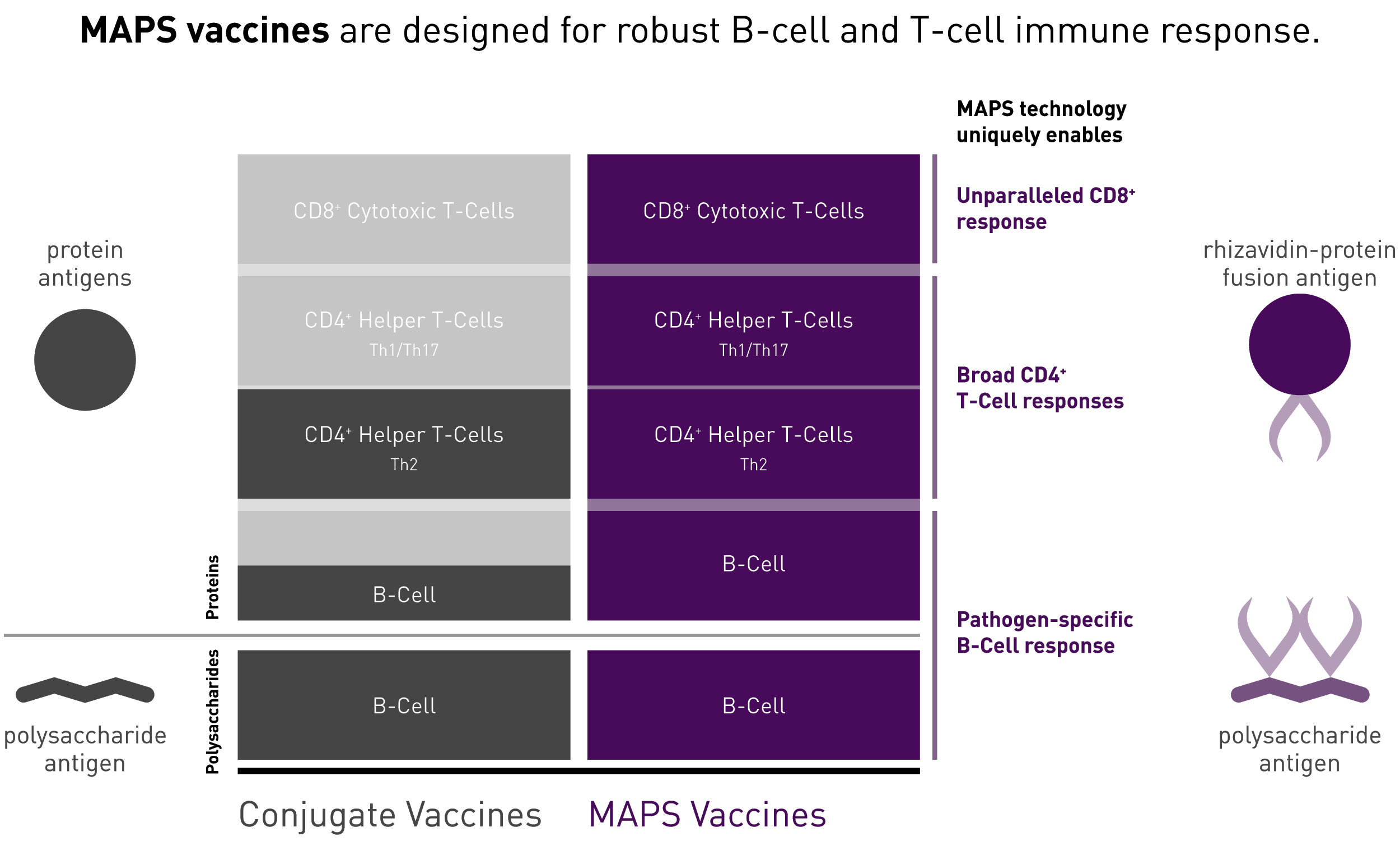
MAPS is turning to a promising approach that combines the efficacy of whole-cell vaccines with the safety and reproducibility of cell-free vaccines. The technology involves two molecules: biotin (vitamin B7) coupled to a polysaccharide component, and the protein rhizavidin, which goes together with the protein antigen. The molecules are closely coupled, with affinity interaction used instead of covalent binding. It is claimed that the technique induces both B- and T-cell responses equally: the immune system recognizes the chemical construct as one large antigen. The efficacy of such vaccines approaches 90%–95%. MAPS vaccine is able to cover up to nine dozen serotypes of S. pneumonia.
The experimental pneumococcal MAPS vaccine ASP3772, which has completed a phase 2 clinical trial, has proven to be protective. ASP3772 includes 24 pneumococcal polysaccharides and two conserved pneumococcal proteins.
Vaxcyte
An interesting approach to pneumococcal vaccine development is being taken by Vaxcyte, formerly SutroVax, which has already received $284.5 million in funding.
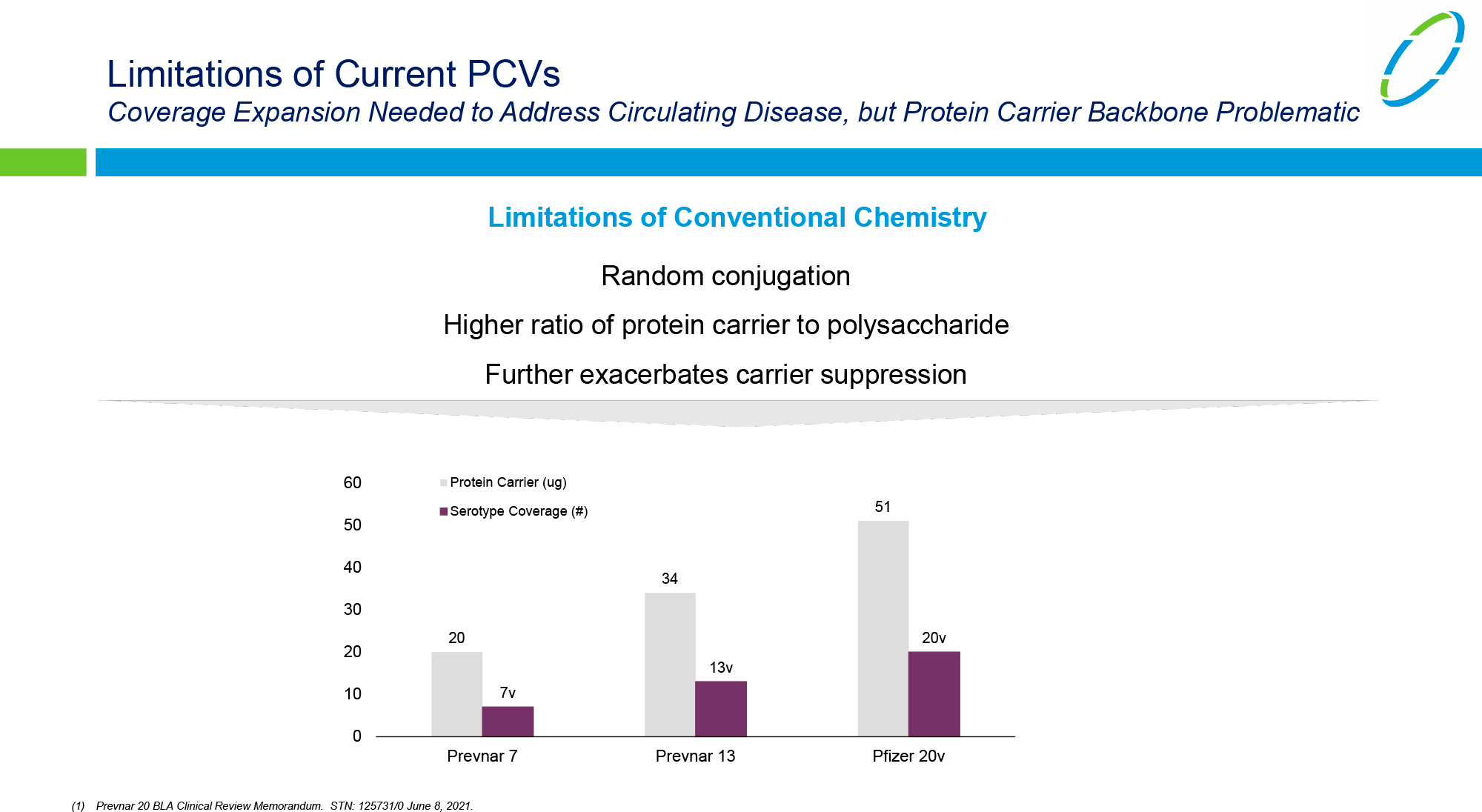
Conjugated vaccines are really difficult to produce. For example, a 20-valent vaccine product means that we are dealing with 20 separate conjugate vaccines mixed together. Each conjugate uses the same protein carrier with different polysaccharides that generate protective antibodies against a particular pneumococcal serotype.
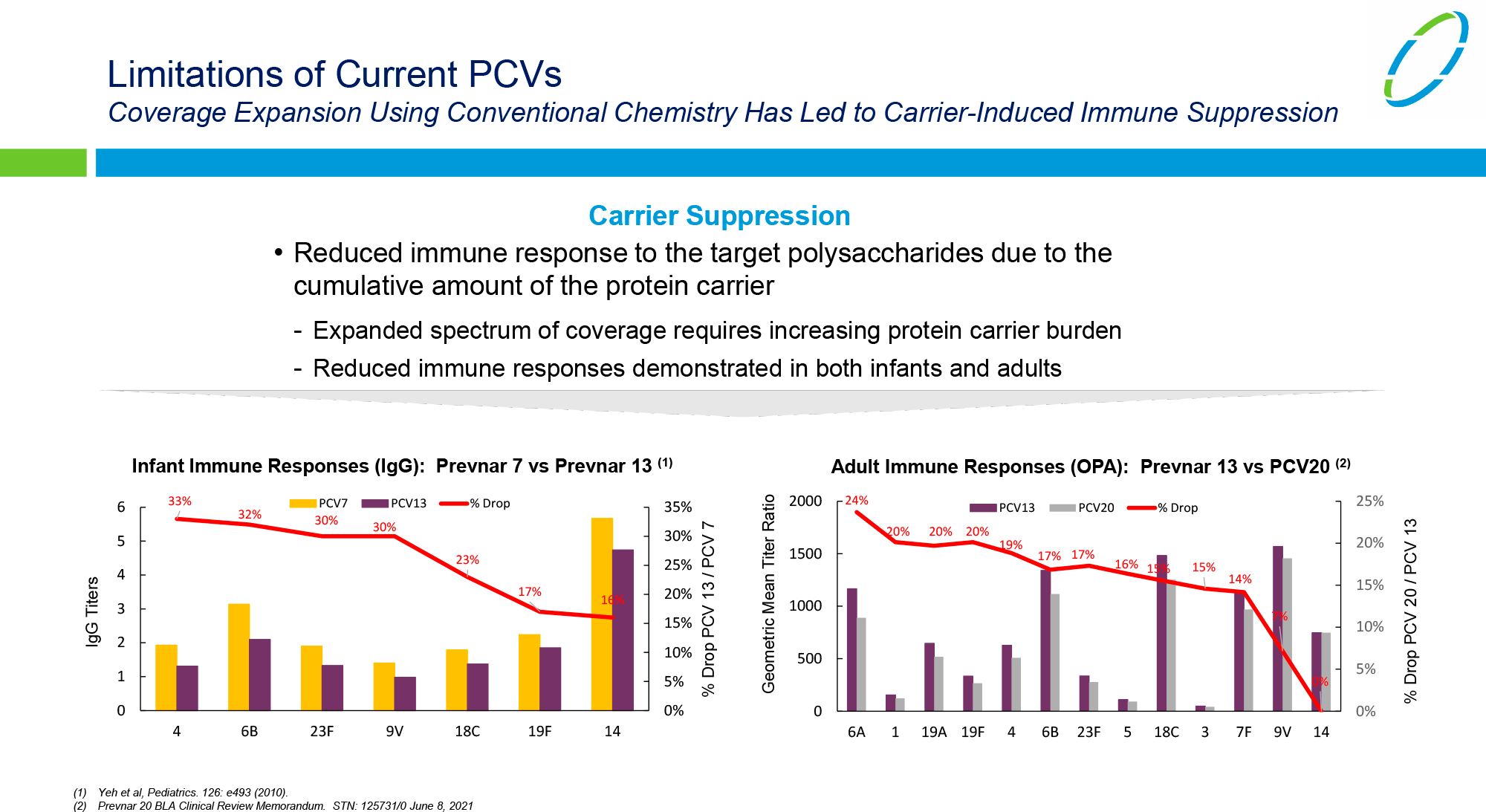
The technical difficulty arises because as new serotypes are added, it becomes increasingly difficult for the vaccine to elicit a sufficiently strong immune response. Each additional valent means more carrier protein, detoxified diphtheria toxin, which ultimately attracts the attention of more CD4+ T cells, which inevitably takes away their ability to develop a secondary immune response against the respective pneumococcal serotypes and reduces the effectiveness of the vaccine.
- It is appropriate to draw a parallel with making 20 different sandwiches: ham, chicken, butter, and peanut paste, etc., all with bread in common. So, if you eat all these sandwiches, there will be an overabundance of bread. The Prevnar 20 and Vaxneuvance vaccines essentially require the immune system to eat 20 and 15 sandwiches, respectively. This is a heavy load for it, a distraction from the pneumococcal defense itself.
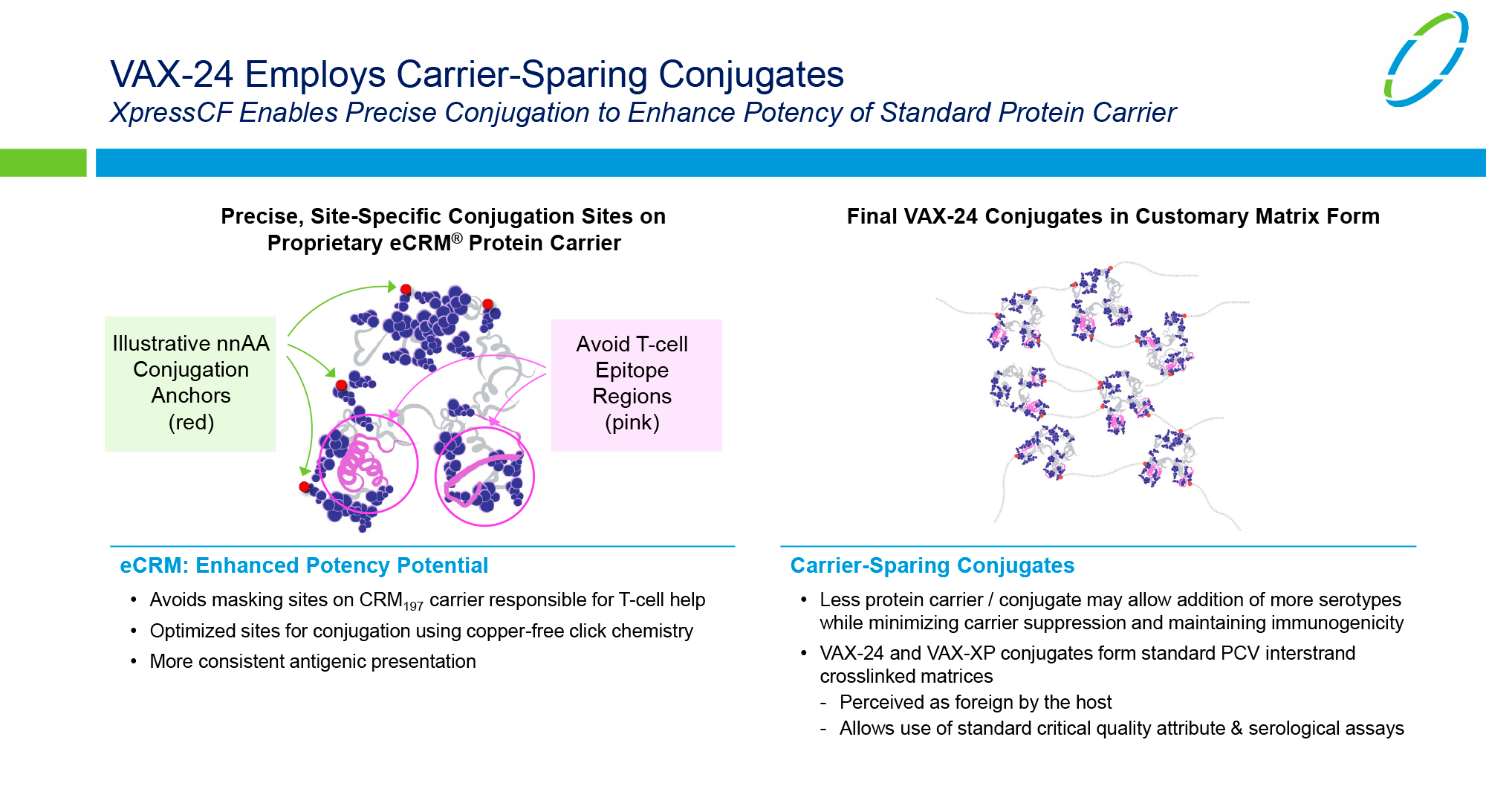
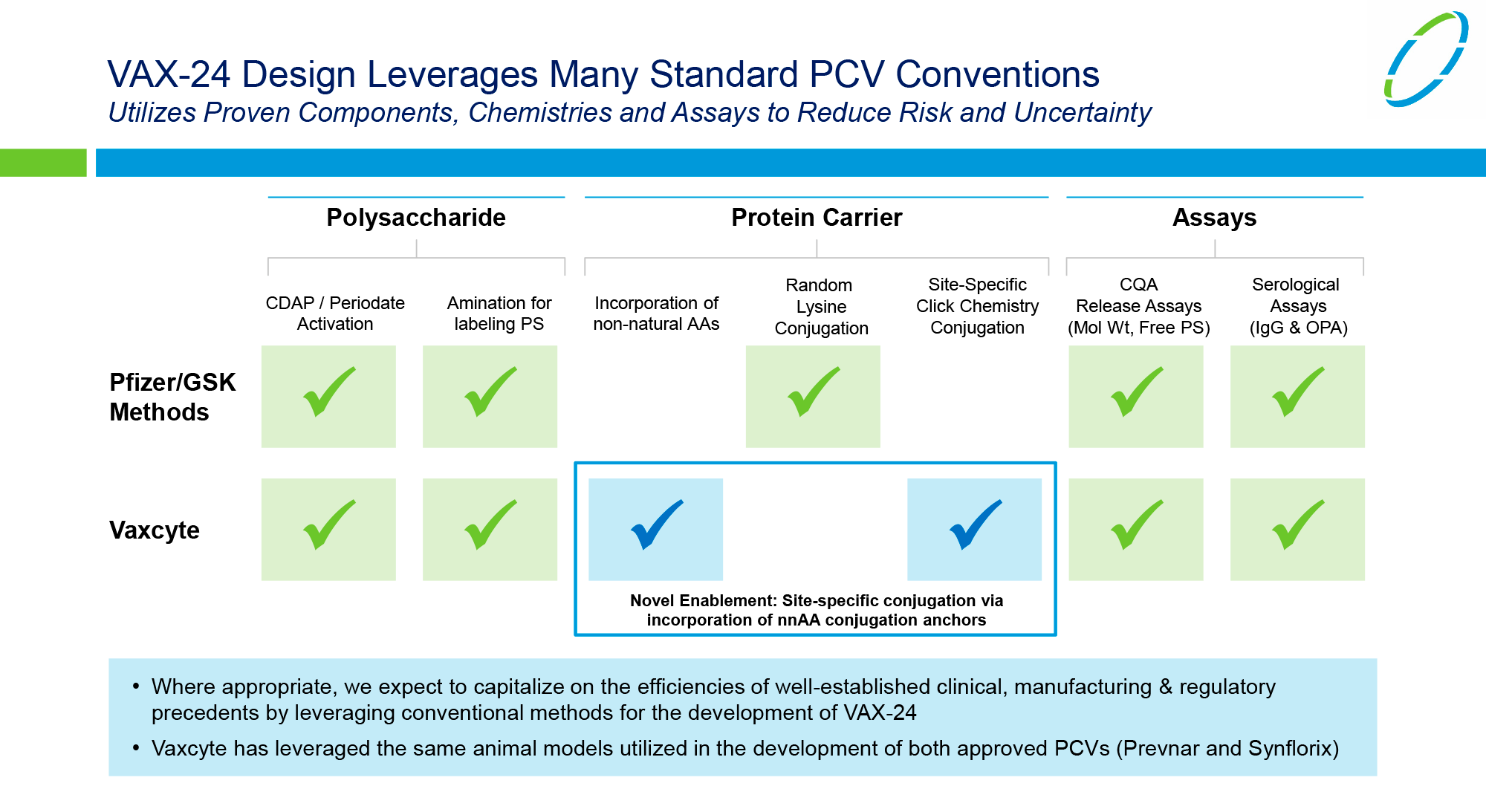
Vaxcyte turned to an elegant solution. Using the Xpress CF cell-free protein synthesis platform licensed from Sutro Biopharma, it was possible to precisely site polysaccharide conjugates on the protein carrier by including non-native amino acids (nnAAs) as covalent conjugation anchors. First, the amount of diphtheria toxin diverting the attention of the immune system away from the disease-specific antigen was significantly reduced. Second, masking sites on the carrier protein were avoided — in contrast to Pfizer’s and Merck & Co.’s pneumococcal vaccines, in which polysaccharides are conjugated randomly, covering some primary T cell epitopes and reducing immunogenic potential.
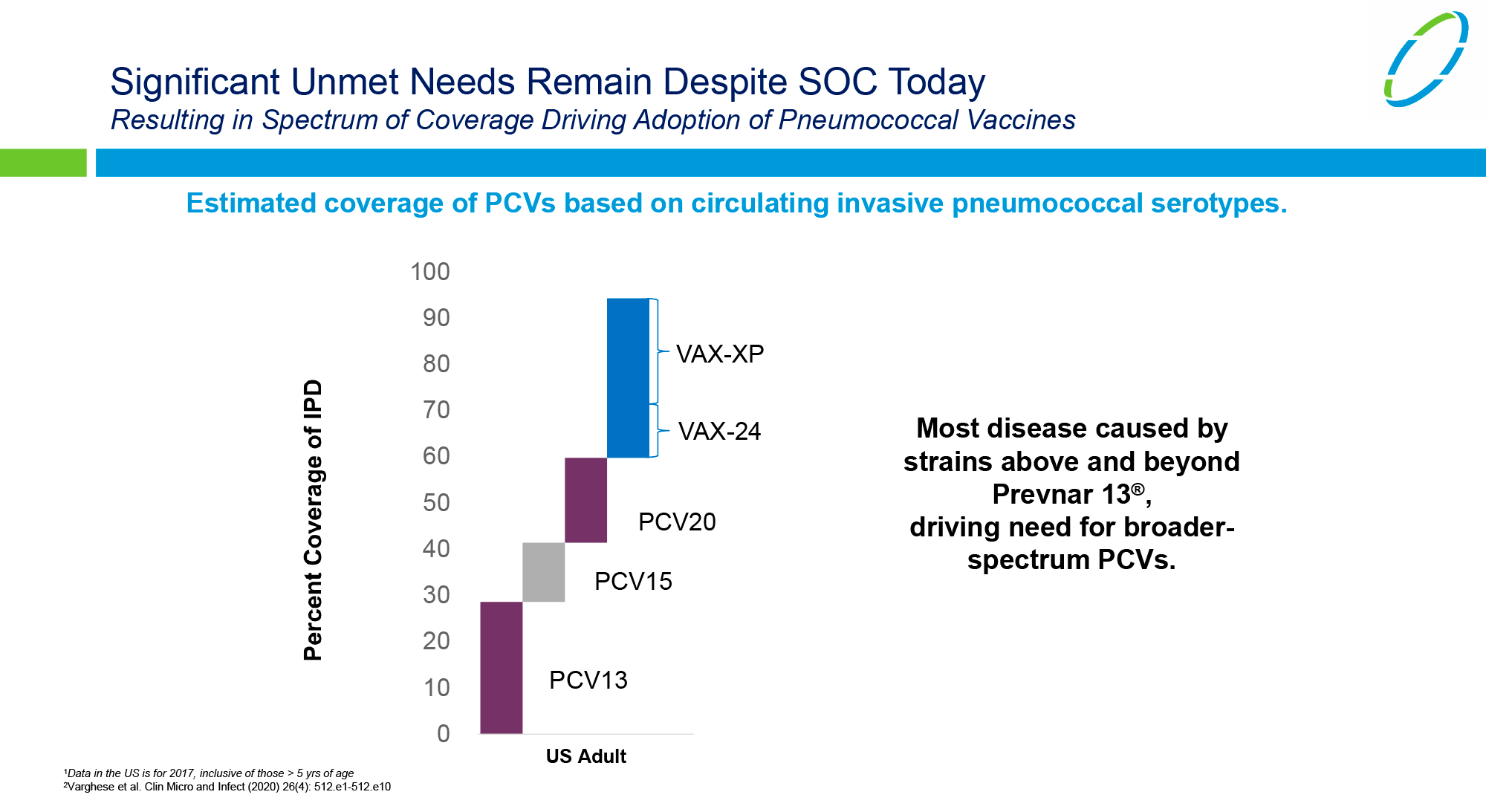

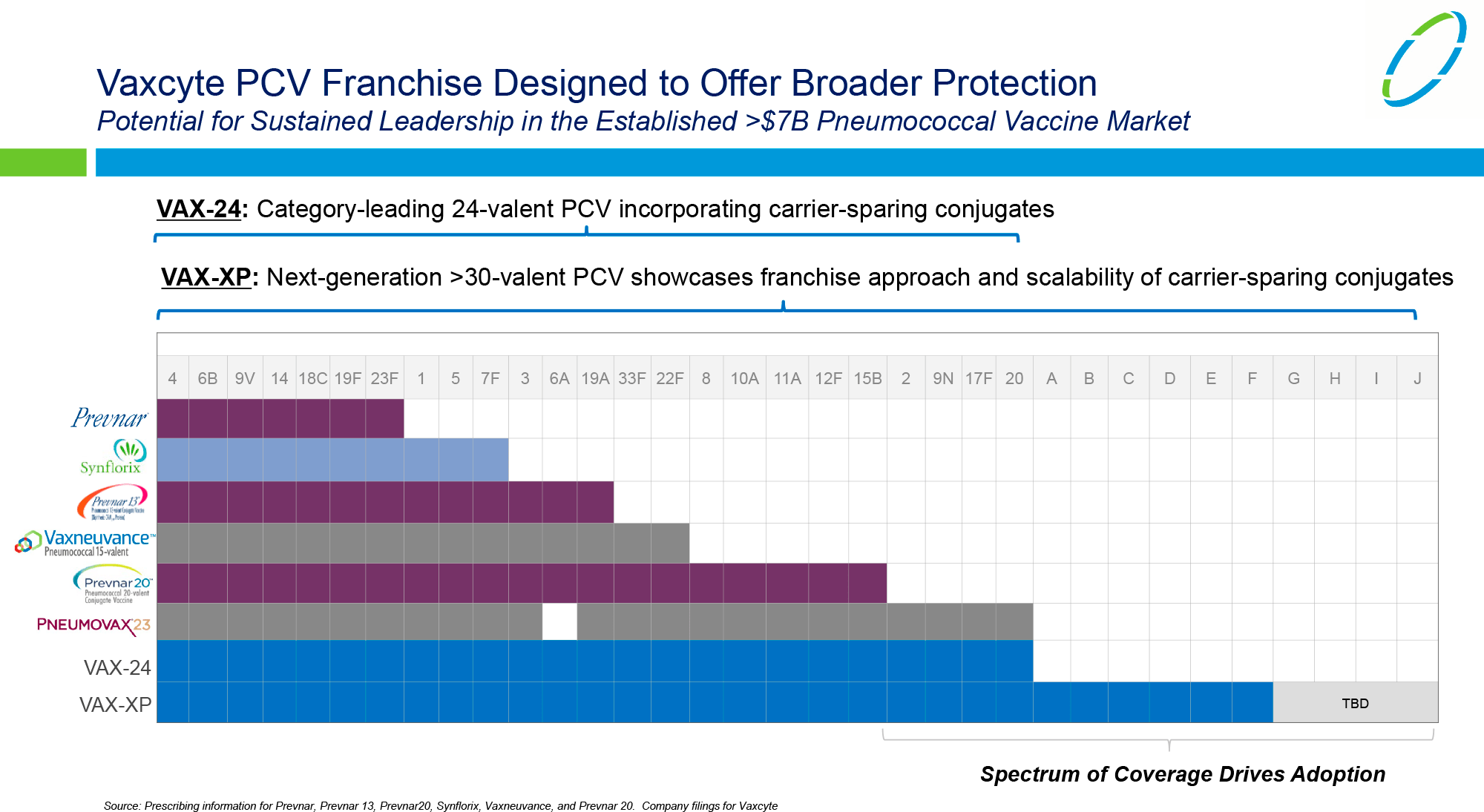

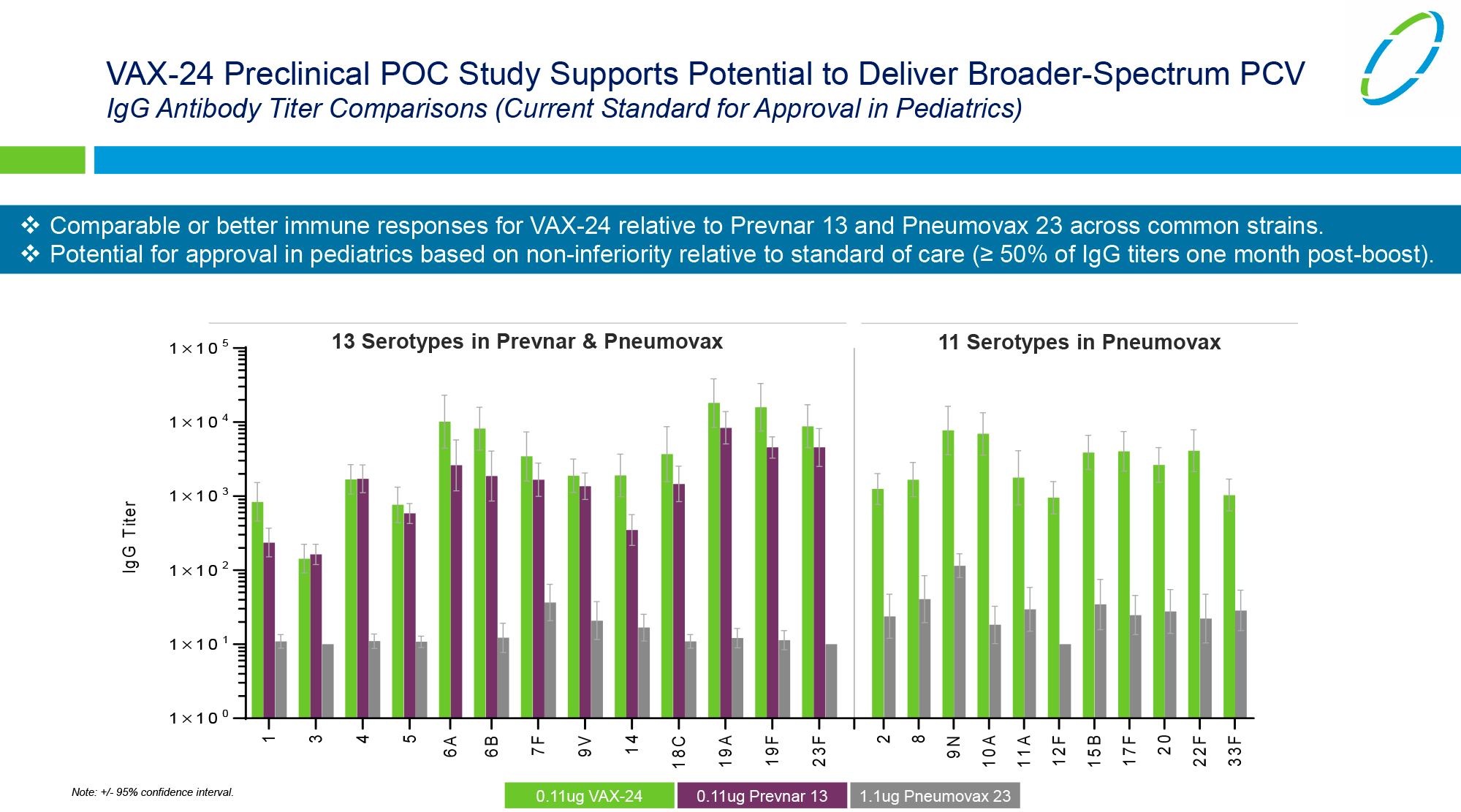
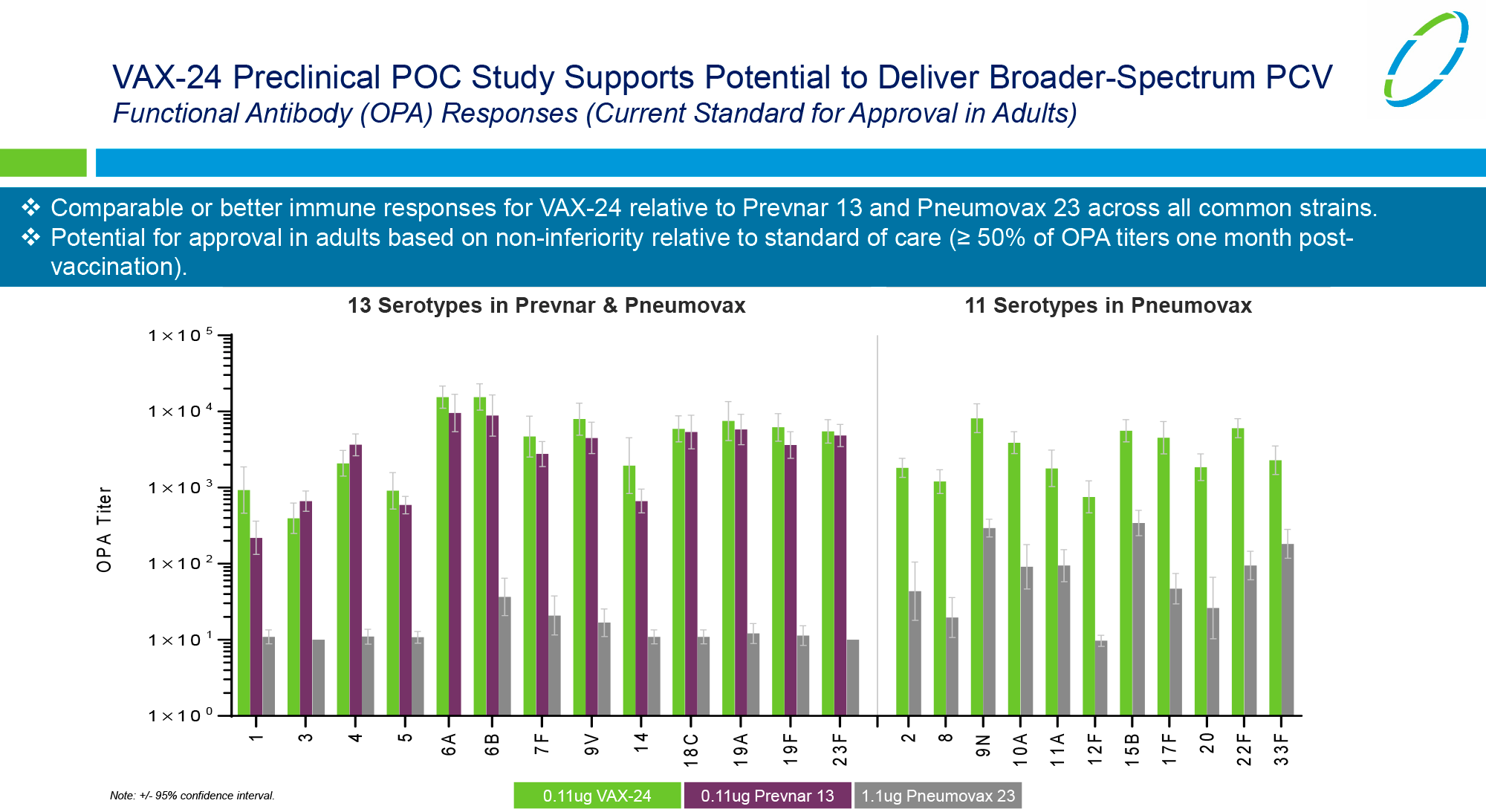
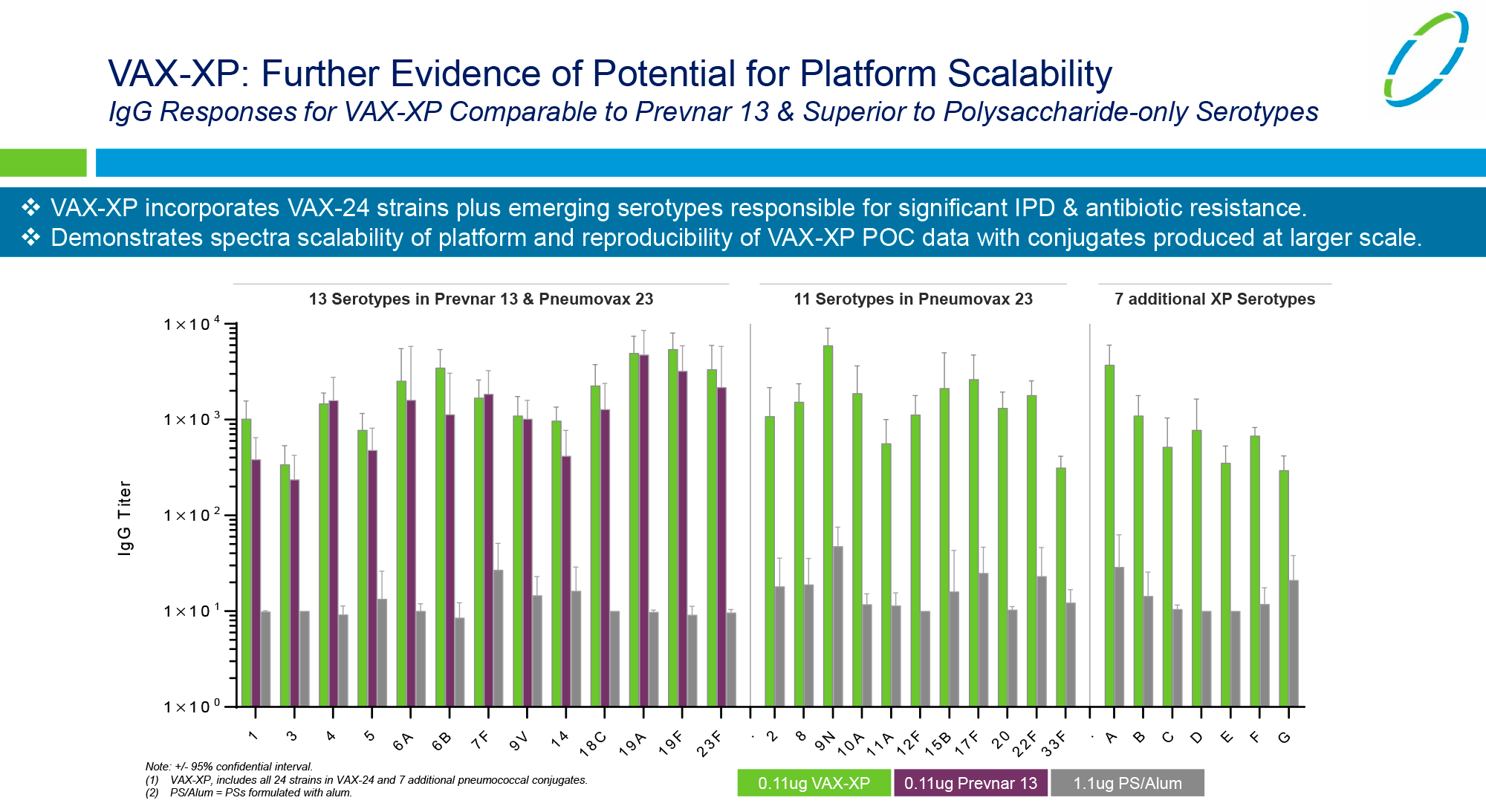
Vaxcyte’s lead vaccine candidate is the 24-valent pneumococcal vaccine VAX-24, with a clinical trial scheduled for launch in the first half of 2022. Going forward, Vaxcyte intends to throw its energies into the development of VAX-XP, which will provide protection against at least 30 serotypes of S. pneumonia.
Inventprise
Inventprise, backed by money from the Bill & Melinda Gates Foundation, is working on an experimental 25-valent pneumococcal vaccine, IVT-25. Inventprise’s proprietary scalable conjugation technology uses a hydrazide—polyethylene glycol (PEG)—hydrazide linker designed to create specific, highly immunogenic, and conjugated broad-spectrum vaccines. The technology solves the problem of reduced immunogenicity observed with high-valent pneumococcal conjugate vaccines and does so by increasing the availability of antigenic polysaccharide epitopes. The linker also improves carrier function and suppresses the immune response to it through steric shielding.