WHAT HAPPENED
Nexsheld (sipavibart) is a new drug indicated for pre-exposure prophylaxis (PrEP) of coronavirus disease (COVID-19) caused by SARS-CoV-2 virus in adults and adolescents (12 years and older weighing at least 40 kg).
Nexsheld is used only if the individual is, first, not currently infected with SARS-CoV-2 and has not had contact with an infected SARS-CoV-2 persons in the recent past and, second, is characterized by moderate-to-severe immune compromise due to a medical condition, immunosuppressive medication, or any treatment and is therefore unlikely to mount an adequate immune response to COVID-19 vaccination.
Nexsheld is administered by intramuscular injection once every six months.
Sipavibart was developed by AstraZeneca to replace the now-defunct Evusheld (tixagevimab + cilgavimab), which was the first drug indicated for COVID-19 PrEP, but which quickly lost its effectiveness due to the emergence of new Omicron variants of SARS-CoV-2.
Nexsheld’s filing is scheduled to be submitted to regulators in the first half of 2024.
Nexsheld is a hypothetical brand name for sipavibart.

Pemgarda: For COVID-19 Protection Instead of Vaccines
Pemivibart every three months. For those who cannot receive the COVID-19 vaccine.
WHY IT MATTERS
Real-world clinical evidence suggests that people with compromised immunity experience a disproportionate burden of COVID-19 compared to the general population, being much more likely to experience a severe course of disease and its adverse outcomes.
Thus, the INFORM observational population-based study of UK residents found that immunocompromised individuals face a significantly higher risk of hospitalization or death due to COVID-19 complications. For certain categories, these risks are 13 and 20 times higher. Although they account for only 3.9% of the population, they significantly contribute to the statistics of poor COVID-19 outcomes. In 2022, immunocompromised persons accounted for 22% of hospitalizations, 28% of ICU admissions, and 24% of deaths. This is notwithstanding that 84% of immunocompromised people have received at least three doses of COVID-19 vaccines [1].
The EPOCH-US observational cohort study of U.S. residents conducted between April 2020 and March 2022 found that immunocompromised individuals, who make up 2.7% of the general population, require over four times as many healthcare resources when hospitalized with COVID-19 [2].
CLINICAL VALIDATION
The SUPERNOVA (NCT05648110) phase 3 (randomized, double-blind, placebo-controlled and active-controlled, multicenter,international) clinical trial enrolled volunteers (n=3200) aged 12 years and older to study the efficacy and safety of Nexsheld (sipavibart) versus Evusheld in the COVID-19 pre-exposure prophylaxis.
Key eligibility requirements include a negative rapid test for COVID-19 antigen and immunocompromised status for a reason such as solid or hematologic malignancy, solid organ or hematopoietic stem cell transplant, receiving immunosuppressive drugs, CAR T-cell therapy or depleting B-cell pool therapy, hemodialysis, or moderate or severe primary immunodeficiency.
Participants received intramuscular injections of Nexsheld 300 mg, Evusheld 600 mg, or placebo twice at 6-month interval.
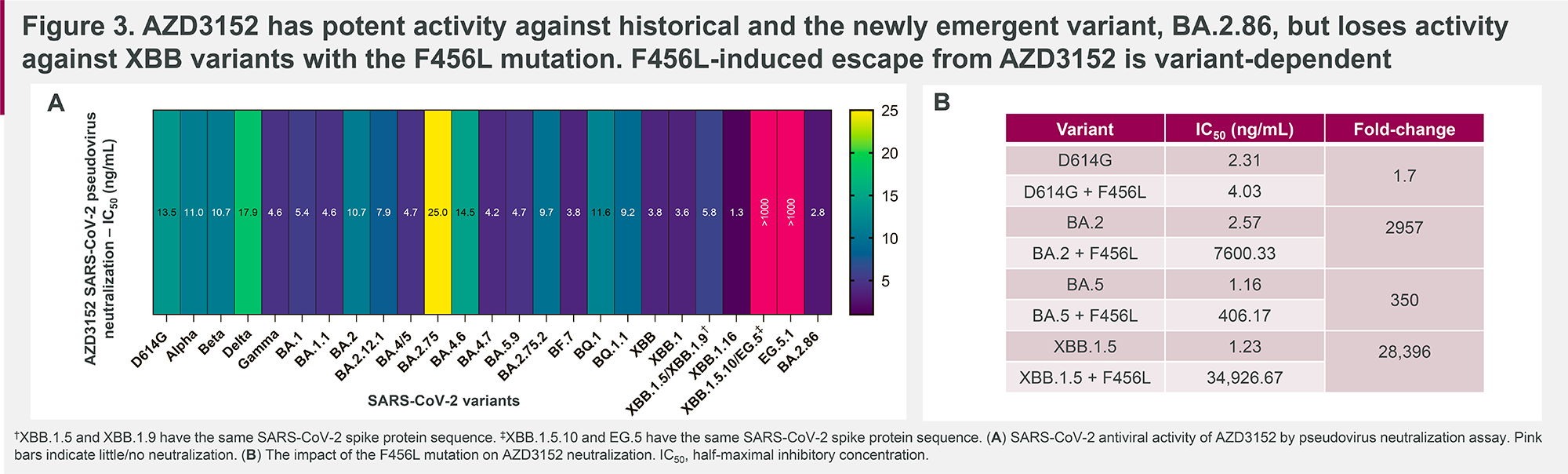
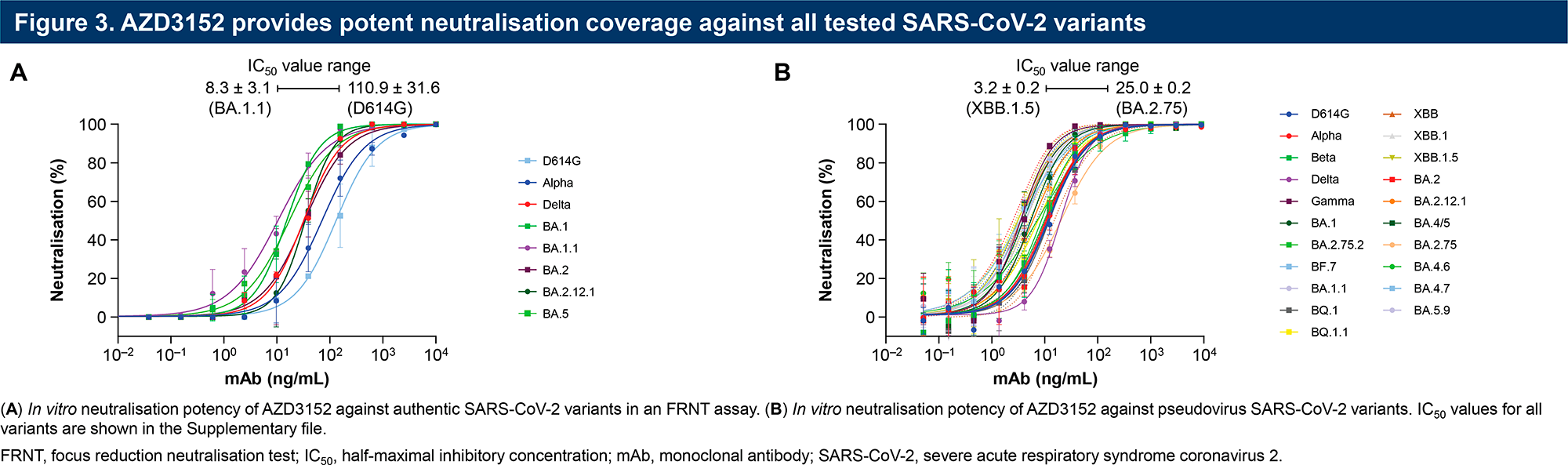
During a one-year period, the neutralizing activity of Nexsheld and Evusheld and their efficacy in preventing the development of symptomatic COVID-19 caused by any variant of SARS-CoV-2 and its variants without the F456L mutation were comparatively evaluated. Data regarding cases of symptomatic COVID-19, severe disease, hospitalization due to complications, and deaths were also collected.
The study, which began in mid-December 2022, was to be completed in early September 2023. It remains to wait for the publication of its results.
THE EFFECTIVENESS
During the development of Nexsheld (sipavibart), the primary goal was to make this monoclonal antibody in such a way that its neutralizing activity would remain as high as possible against, first, the previously dominant variants of SARS-CoV-2 and, second, its new variants, which are becoming more and more widespread nowadays.
And if the first part of this task is quite realizable, the second part is inevitably difficult, because SARS-CoV-2 undergoes a non-stop process of evolutionary genetic changes that can potentially reduce the effectiveness of any prophylactic or medicinal product or turn it into a non-working one.
This is why it cannot be stated unequivocally that sipavibart can provide absolute protection against COVID-19. Nevertheless, some reliable assumptions can still be made, even without the results of the clinical trial of Nexsheld being ready.
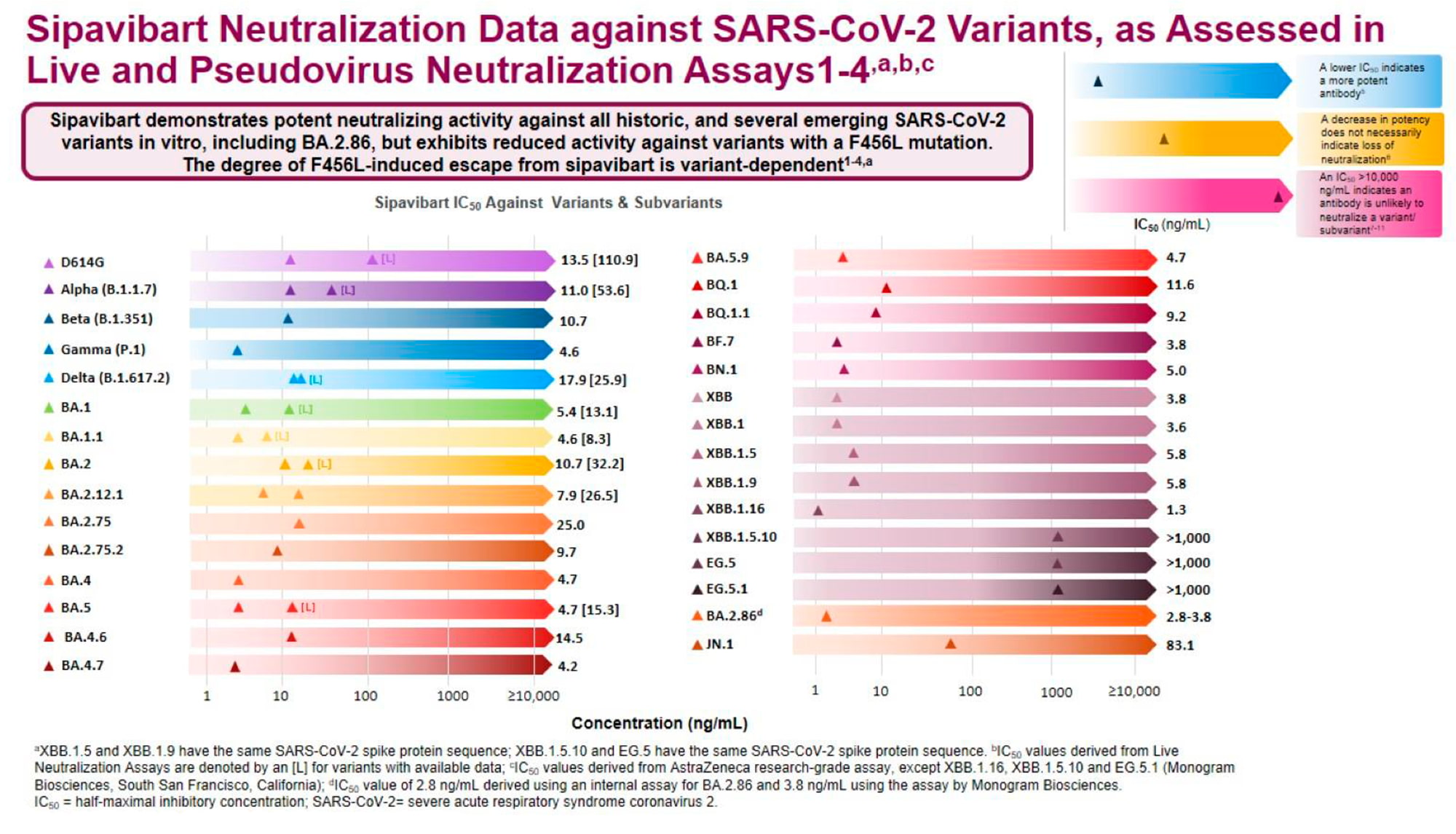
Thus, if we take into account that BA.2.86, one of the Omicron variants is now dominant throughout the planet, then sipavibart will certainly provide adequate protection, but will be useless in the case of the not so long ago leading Omicron variant XBB.1.5, if this strain has a resistance mutation F456L.
To better understand the degree of protective efficacy of Nexsheld and to make an informed decision as to whether its prophylactic use is justified, the following data sets should be reviewed:
- World Health Organization (WHO) tracking of currently circulating SARS-CoV-2 variants of interest (VOIs) and variants under monitoring (VUMs) [1]
- As of early February 2024, the VOIs are as follows: XBB.1.5 (23A), XBB.1.16 (23B), EG.5, BA.2.86 (23I), and JN.1
- As of late January 2024, the VUMs are as follows: XBB (22F), XBB.1.9.1 (23D), and XBB.2.3 (23E).
- The prevalence of a particular SARS-CoV-2 variant in a specific region or country [2] [3] [4] [5] [6].
- Databases accumulating information on the decreased susceptibility of SARS-CoV-2 variants to the neutralizing activity of monoclonal antibodies [7].
- Relevant presentation, academic and research publications.
- Prescribing information for Nexsheld (sipavibart), which should include details regarding neutralization of SARS-CoV-2 variants with data on decreased susceptibility and resistance.
THE COST
The cost of Nexsheld (sipavibart) will be announced when the drug receives regulatory authorization.
It is safe to assume that the price of Nexsheld will in no way be set below $2,000. This is a typical price for anti-SARS-CoV-2 monoclonal antibodies when they were still effective and universally authorized for use [1] [2] [3] [4] [5].
For AstraZeneca’s business, the launch of Nexsheld is definitely profitable if we build on the earnings of the bygone Evusheld, which brought in $85 million, $2.19 billion, and $312 million in 2021, 2022, and 2023, respectively.
HOW IT WORKS
Sipavibart (AZD3152) is a fully human IgG1 monoclonal antibody that target a highly conserved epitope on the receptor-binding domain (RBD) of the SARS-CoV-2 spike protein.
When sipavibart binds to RBD, it prevents the interaction between RBD and angiotensin-converting enzyme 2 (ACE2), a receptor that SARS-CoV-2 uses to attach to the host cell membrane and enter the cell.
Passive immunization with sipavibart against COVID-19, assuming neutralization of SARS-CoV-2, provides temporary protection against infection, and if infection does occur, a slowing of disease progression and accelerated recovery should be expected.
Sipavibart is an antibody derived from memory B cells of a recovered patient who had been vaccinated but still encountered COVID-19 caused by the Omicron variant BA.1 of SARS-CoV-2.
Amino acid substitutions have been introduced into the sipavibart antibody scaffold to enhance its pharmacokinetic and biochemical properties [1]. Thus, the YTE substitution increased the antibody’s affinity to the neonatal Fc receptor, resulting in improved recycling and a significantly prolonged half-life of the drug so that the duration of its action more than tripled compared to conventional non-optimized antibodies [2] [3] [4].
The prolonged persistence of sipavibart in the body suggests that protection against COVID-19 is maintained for at least six months after a single dose of the drug [5]. However, due to the highly mutational nature of SARS-CoV-2, sipavibart may need to be administered more frequently to achieve maximum COVID-19 protection.
The TM amino acid substitution resulted in a decrease in binding potency to FcγR and C1q, reflected by a significant weakening or even absence of effector Fc function, including antibody-dependent cellular phagocytosis (ADCP), antibody-dependent cellular cytotoxicity (ADCC), antibody-dependent complement deposition (ADCD), and antibody-dependent natural killer cell activation (ADNKA). The potential risk of antibody-dependent enhancement (ADE), a phenomenon in which suboptimal virus-specific antibodies promote rather than suppress infection or disease, is minimized [6].
PERICULUM IN MORA
In early December 2021, Evusheld (tixagevimab + cilgavimab), a monoclonal antibody combination by AstraZeneca, became the first (and only) PrEP for prevention of COVID-19 in those who are ineligible or contraindicated for vaccination.
The emergence of Evusheld was a significant event, listed by Time magazine as one of the best inventions of 2022 [1] [2].
However, at the end of January 2023, the FDA canceled the Evusheld authorization. Due to the abundance of new Omicron variants of SARS-CoV-2, which it is unable to cope with, this method of protection against infection no longer works [3].

Evusheld: First Drug for Strong and Long-Lasting Protection Against Coronavirus
One dose of AstraZeneca’s monoclonal antibody cocktail protects against COVID-19 for six months or longer.
Other pharmaceutical developers have failed to provide an alternative to Evusheld, leaving tens of millions of people in desperate need of passive immunization against COVID-19, instead of active immunization through vaccination.
AstraZeneca, obviously predicting the sad fate of Evusheld, in advance, in mid-May 2022 licensed sipavibart and other anti-SARS-CoV-2 monoclonal antibodies from the British RQ Bio and in return promised up to $157 million plus royalties from the sale of the finished drug [2].
Clinical trial of sipavibart began in mid-December 2022 [3].
AstraZeneca anticipated making sipavibart available for widespread use in the second half of 2023 [4].
Absolutely all conditions were in place to quickly bring Nexsheld (sipavibart) to the open market, as the drug adopted exactly the same deeply optimized antibody scaffold on the basis of which Evusheld was built, i.e. no constructive modifications were required. In fact, the only task was to clinically evaluate the protective efficacy of sipavibart against new SARS-CoV-2 variants, which no longer responded to Evusheld.
But it wasn’t meant to be.
In mid-March 2024, Invivyd launched Pemgarda (pemivibart), a monoclonal antibody indicated for pre-exposure prophylaxis (PrEP) of COVID-19 in adults and adolescents.
Pemgarda: For COVID-19 Protection Instead of Vaccines
Pemivibart every three months. For those who cannot receive the COVID-19 vaccine.
THE FLIPSIDE
In contrast to the United States [1], several territories, including Europe, the UK, Canada, Australia, and Russia, continue to incorporate Evusheld and/or other anti-SARS-CoV-2 monoclonal antibodies and combinations thereof into their clinical guidelines for the prevention and/or treatment of COVID-19 [2] [3] [4] [5] [6].
Remarkably, regulators themselves have long issued numerous warnings about the lack of efficacy of monoclonal antibodies against new SARS-CoV-2 variants in the Omicron lineages era, however have not yet revoked their marketing authorizations [7] [8] [9] [10]. It is possible that industry watchdogs are adopting a wait-and-see approach: What if the coronavirus mutates so that monoclonal antibodies become effective again?
Authoritative medical agencies have spoken out strongly against any anti-SARS-CoV-2 monoclonal antibodies because of their complete lack of proper efficacy: SARS-CoV-2 has mutated too deeply and severely for these drugs, which previously worked, to continue to provide the necessary antiviral neutralizing activity [11] [12] [13].
According to a database maintained by Stanford University that tracks the decreasing susceptibility of SARS-CoV-2 variants to monoclonal antibodies targeting the virus’s spike protein, the outlook is grim. These drugs are not at all suitable for the war against COVID-19 with its current set of mutations [14].
Apart from Pemgarda (pemivibart), none of the ever formally authorized anti-SARS-CoV-2 monoclonal antibodies, even if previously relatively successful in the prevention (pre- and post-exposure) and treatment of COVID-19, make any sense to use now. Currently, the following drugs are considered completely useless [15] [16] [17] [18] [19] [20] [21] [22] [23] [24]:
- amubarvimab (BRII-196, P2C-1F11) + romlusevimab (BRII-198, P2B-1G5)
- bamlanivimab (LY3819253, LY-CoV555) + etesevimab (LY3832479, LY-CoV016, JS016, CB6)
- bebtelovimab (LY-CoV1404, LY3853113)
- casirivimab (REGN10933) + imdevimab (REGN10987) — marketed under the brand name REGEN-COV/Ronapreve
- regdanvimab (CT-P59) — Regkirona
- sotrovimab (VIR-7831, GSK4182136) — Xevudy
- tixagevimab (AZD8895, COV2-2196) + cilgavimab (AZD1061, COV2-2130) — Evusheld (AZD7442).
The position of evidence-based medicine is clear: Do not spend money on absolutely worthless drugs drugs while falsely reassuring people that they are protected against COVID-19.