In January 2021, Eli Lilly reported that the experimental drug donanemab had successfully passed a clinical trial in the therapy of patients with early-stage Alzheimer’s disease. The administration of donanemab has been shown to significantly inhibit the processes associated with cognitive decline and the ability to perform activities of daily living.
On the wave of good news, Eli Lilly’s stock price added 14% at once determining a $23 billion increase in the market value of the U.S. pharmaceutical company.
In March 20201, Eli Lilly disclosed the details of a relevant clinical trial which gave the patient and physician community new hope. No, there is still no talk of victory over Alzheimer’s disease. At this moment, we are only talking about the fact that the upcoming drug is able to delay the onset of severe dementia which in the end leads to insanity and incapacitation of literally every person suffering from this neurodegenerative disease.
In any case, donanemab will have to undergo additional and lengthy validation which will definitively establish how effective and safe it is.
The latest innovation for Alzheimer’s disease therapy is Oligomannate (sodium oligomannate), proposed by China’s Shanghai Green Valley Pharmaceuticals and made from brown algae. The idea was to modulate the gut microbiota in favor of getting rid of microglial-mediated neuroinflammation and amyloidosis.

Oligomannate: Finally New Drug to Treat Alzheimer’s Disease
Innovative Chinese medicine eliminates gut microbiota dysbiosis, and it helps slow the progression of dementia in Alzheimer’s disease.
Donanemab and Alzheimer’s Disease Therapy: Efficacy and Safety
The TRAILBLAZER-ALZ (NCT03367403) phase II clinical trial (randomized, double-blind, placebo-controlled, multicenter) enrolled patients (n=272) aged 60–85 years with symptomatic early-stage Alzheimer’s disease.
Among the main inclusion criteria: progressive memory impairment lasting at least 6 months; a score of 20–28 on the Mini-Mental State Examination (MMSE).
Participants were given donanemab (700 mg the first three doses, then 1400 mg) or placebo — intravenously every 4 weeks for 72 weeks.
The primary endpoint, fixed after 76 weeks of treatment, was a change in the integrated Alzheimer’s Disease Rating Scale (iADRS) score. It is a composite score that combines the Alzheimer’s Disease Assessment Scale–Cognitive Subscale (ADAS-Cog-13) and the Alzheimer’s Disease Cooperative Study-instrumental Activities of Daily Living (ADCS-iADL) scores for cognitive function. Simply put, the iADRS reflects the level of thinking and mental abilities along with the ability to live independently in a routine living environment.
Secondary endpoints considered over the same period of therapy included changes on a number of the following scales: ADAS-Cog-13, ADCS-iADL, MMSE, and the Clinical Dementia Rating Scale Sum of Boxes (CDR-SB). In addition, changes in biomarkers such as amyloid beta and tau protein deposits in the brain were studied.
The group of subjects who received donanemab demonstrated statistically significant inhibition of processes associated with cognitive deterioration and the ability to perform independent daily activities. Relative to the placebo group, the candidate drug provided a 32% delay in changes in the primary endpoint.
Thus, while the baseline iADRS score was 106 in both groups (less is worse), at the end of the experimental treatment the least-squares mean change (LSM; henceforward) change in the donanemab group was −6.86 points — versus −10.06 points in the control group; the difference was equal to 3.20 (95% CI: 0.12–6.27) [p=0.04].

Administration of donanemab was reflected by a consistent improvement in all secondary endpoints assessing subjects’ cognitive and functional abilities. However, no nominal statistically significant difference with placebo was found:
- CDR-SB (more is worse): in the donanemab group +1.22 — in the placebo group +1.58, difference −0.36 (95% CI: −0.83 — +0.12)
- ADAS-Cog-13 (more is worse): +2.91 — +4.77, difference −1.86 (95% CI: −3.63 — −0.09)
- ADCS-iADL (less is worse): −3.98 — −5.20, difference +1.21 (95% CI: −0.77 — +3.20)
- MMSE (less is worse): −2.35 — −2.98, difference +0.64 (95% CI: −0.40 — +1.67).

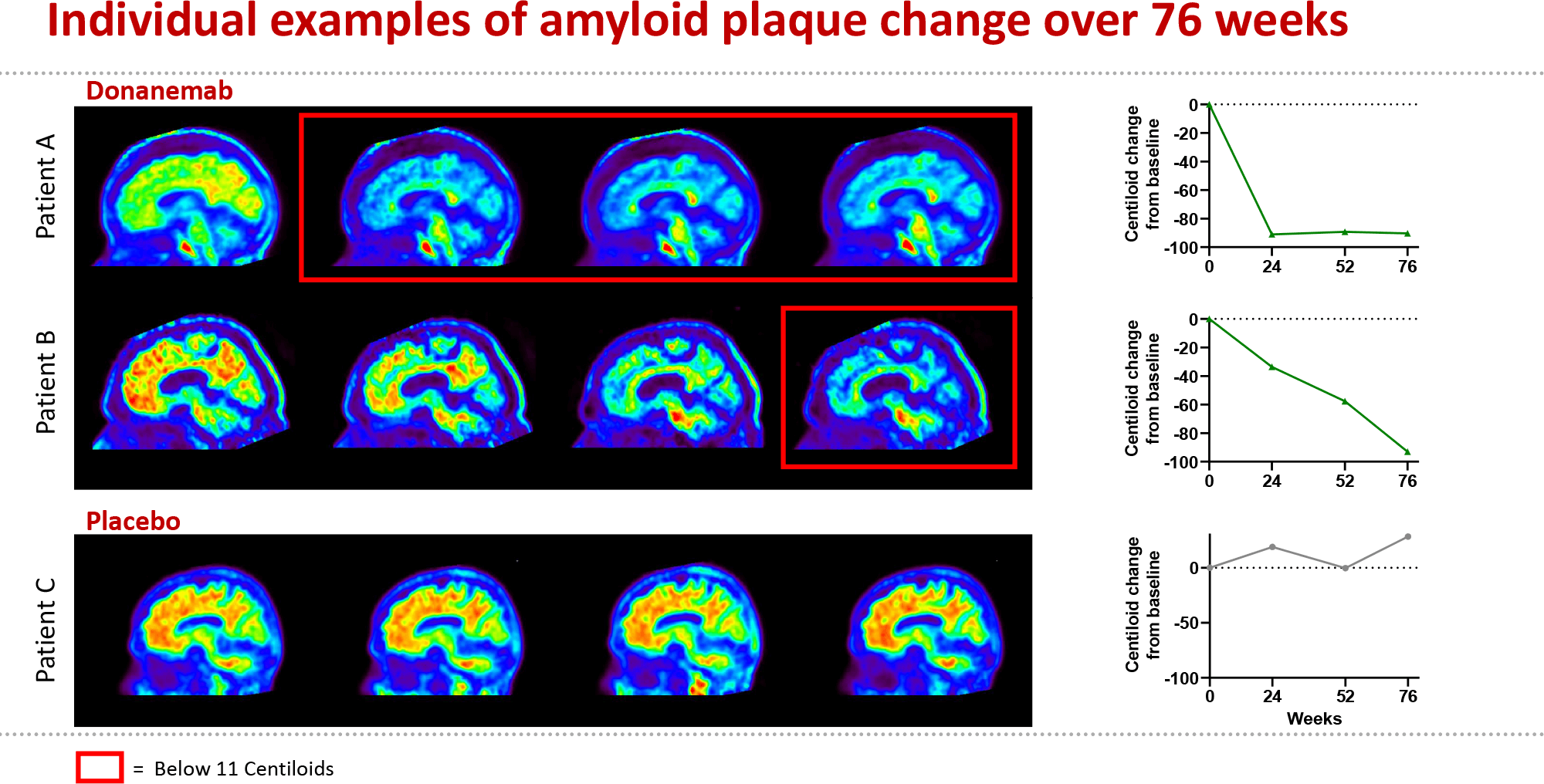
The use of donanemab showed a clear reduction in amyloid load. While its baseline level was 108 and 101 centiloids in the drug and placebo groups, respectively, after treatment it decreased by an average of 85 centiloids and, conversely, added 0.9 centiloids.
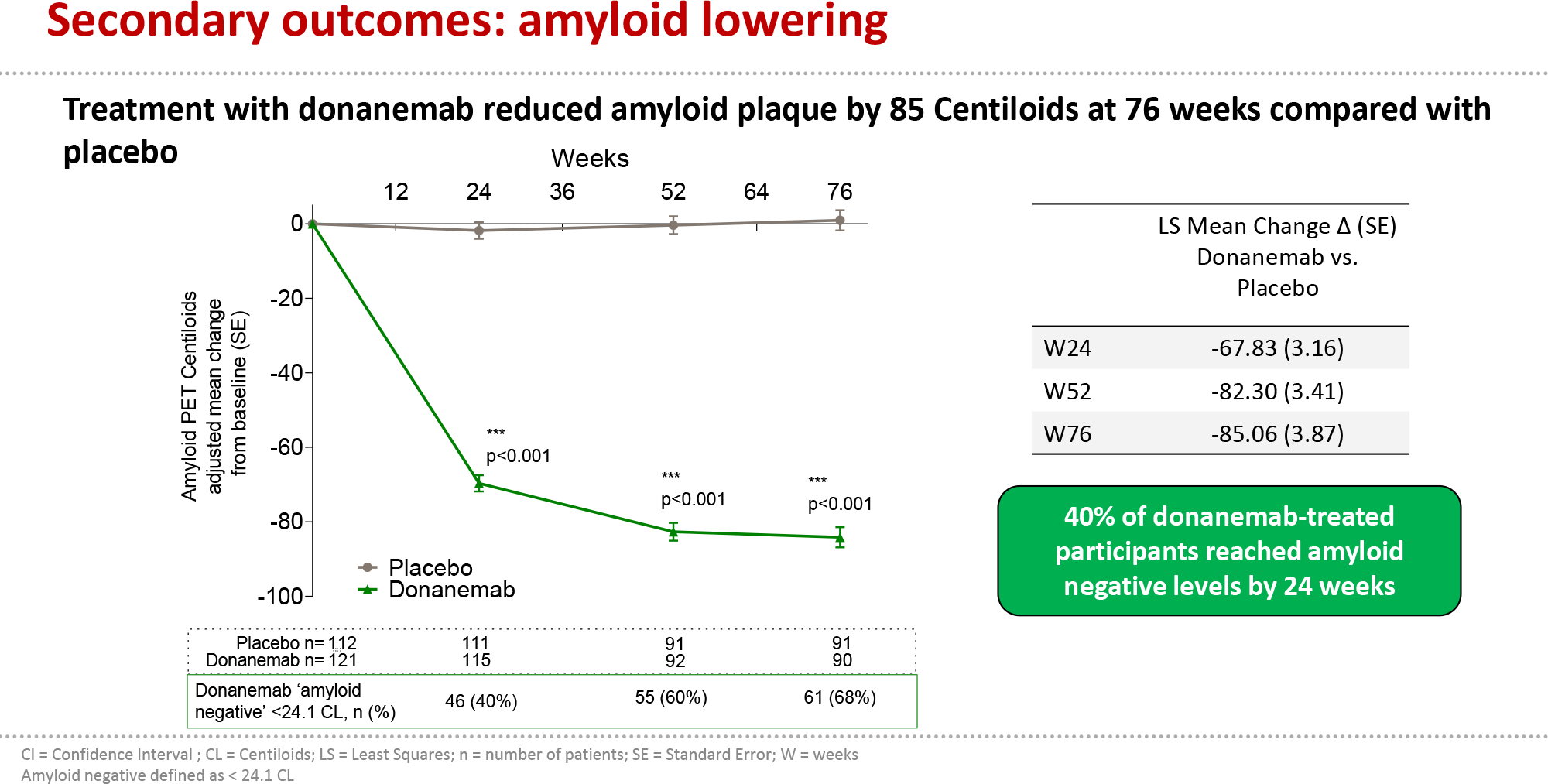
- Centiloid is a standardized measure of the quantitative content of amyloid beta on positron emission tomography (PET) images of the brain. The centiloid scale is broken down from 0 to 100 where 0 is complete absence of amyloid beta deposits (individuals younger than 45 years without Alzheimer’s disease were taken as controls).
- Levels below 25 centiloids indicate the absence of any amyloid beta deposits considered pathological in the setting of Alzheimer’s disease. Therefore, for those patients, whose amyloid load during treatment with donanemab (measured at weeks 24 and 52) fell below 11–25 centiloids, the prescribed dose of the drug was reduced to 700 mg, and for those, whose amyloid load fell either below 11 centiloids in one measurement or below 25 centiloids in two consecutive measurements, donanemab was replaced with placebo.
The proportions of patients in the donanemab group who achieved amyloid-free status at weeks 24, 52, and 76 were 40.0%, 59.8%, and 67.8%.
Administration of donanemab, however, did not result in such a reduction in total tau protein levels as to suggest a significant difference with the control group.

Donanemab administration was echoed in an unusually enhanced reduction in total brain volume and an increase in ventricular volume but not in hippocampal volume, all compared to placebo.
The safety profile of donanemab, while similar to that of other experimental drugs targeting amyloid beta, is characterized by the amyloid-related imaging abnormalities (ARIA) phenomenon. Thus, in the drug group, 26.7% of patients experienced vasogenic cerebral edema (ARIA-E) caused by the release of the proinflammatory cytokine, tumor necrosis factor (TNF). In most cases, this adverse reaction was clinically asymptomatic, nonsignificant (according to MRI images), and resolved on its own (by the median 18 weeks), although it was accompanied by symptomatic manifestations in 6.1% of cases.
Donanemab for Treatment of Alzheimer’s Disease: What’s Next
In parallel, donanemab is being studied in the 18-month TRAILBLAZER-ALZ 2 (NCT04437511) phase II clinical trial (randomized, double-blind, placebo-controlled, multicenter, international) recruiting adult patients (n=500) with symptomatic early-stage Alzheimer’s disease.
Unlike TRAILBLAZER-ALZ, the study does not deny participation to patients with high levels of accumulation of tau protein neurofibrillary tangles. This is due to the fact that increased patient recruitment resulted in increased statistical power thereby allowing the inclusion of individuals with more severe Alzheimer’s disease. In addition, the primary endpoint chosen was change on the familiar CDR-SB scale.
It is possible that even if the interim results of TRAILBLAZER-ALZ 2 prove acceptable, Eli Lilly will proceed to submit a Biologics License Application (BLA) for donanemab to the U.S. Food and Drug Administration (FDA).
The TRAILBLAZER-EXT (NCT04640077) phase II clinical trial (non-randomized, open-label, multicenter) is also ongoing inviting participants from TRAILBLAZER-ALZ which is designed to test the safety and efficacy of donanemab with its long-term use.
Fight Against Alzheimer’s Disease: Mechanism of Action of Donanemab
Accumulation of amyloid beta peptide in the form of amyloid plaques in the brain is an early event in Alzheimer’s disease, presumably leading to neurodegeneration with cognitive and functional impairment. [1][2][3][4] The role of amyloid plaques in pathology progression is supported by the results of studies of rare genetic variants of Alzheimer’s disease in which both growth and reduction of amyloid beta deposits are observed. [5][6] The presence of amyloid plaques in the early stages of the disease increases the likelihood of progression from mild cognitive impairment to dementia. [7] Therapeutic interventions aimed at eliminating amyloid plaques may, it is believed, slow the clinical progression of Alzheimer’s disease.
Another neuropathological sign of Alzheimer’s disease is the presence of intracellular neurofibrillary tangles containing hyperphosphorylated tau protein. According to current models, amyloid beta is responsible for tau pathology, with the complex and synergistic interaction between amyloid beta and tau protein manifesting itself in the later stages of the disease course and making some contribution to its progression. [8]
Donanemab (LY3002813, N3pG) is a humanized monoclonal IgG1 antibody that recognizes the pyroglutamate form of beta-amyloid (pGluAβ), Aβp3–42. This form is the core of amyloid plaques in the brain.
Donanemab, by binding Aβp3–42, activates microglia that performs clearance (elimination) of amyloid beta deposits, and does so without the microhemorrhagia that are common in Alzheimer’s disease immunotherapy.
Most experimental monoclonal antibodies against amyloid beta (failed or still under development) target its soluble or insoluble forms and lack any acceptable affinity for amyloid beta deposits. Donanemab has done things differently: the therapeutic rationale for targeting Aβp3–42 lies in the task of clearing existing amyloid beta plaques from the brain — rather than preventing new ones from forming and growing.
In preclinical studies, combined therapy with donanemab with LY2811376, a beta-secretase 1 (BACE1) inhibitor, was shown to determine 86% clearance of amyloid beta from the brains of PDAPP-transgenic mice — compared with approximately 50% when each drug was used alone. Donanemab eliminated both nuclear and diffuse amyloid beta plaques.
By the way, initially TRAILBLAZER-ALZ actually evaluated a combination of donanemab and LY2811376 but Eli Lilly later abandoned it switching completely to monotherapy: for nothing, none of the many experimental BACE1 inhibitors had ever proven themselves.
Donanemab for Treatment of Alzheimer’s Disease: Expert Comments
The TRAILBLAZER-ALZ clinical trial was only technically successful. The experimental donanemab showed that it is going in the right direction but the data collected are categorically insufficient for principled conclusions about the therapeutic feasibility of eliminating amyloid beta from the brains of patients with Alzheimer’s disease. And so we will have to wait until 2023 when the TRAILBLAZER-ALZ 2 clinical trial ends.
Biogen is known to be eager to get regulatory approval for its aducanumab which similarly targets amyloid beta. If the regulator goes along, the bar for the effectiveness of any of the drugs under development to treat Alzheimer’s disease will drop dramatically, because aducanumab has been more than controversial in terms of its therapeutic effect: its effect is at its limit. In other words, approval of aducanumab would automatically mean approval of donanemab and similar anti-amyloid therapeutic molecules.
Donanemab and aducanumab for Alzheimer’s disease treatment: cross-trial comparison of clinical efficacy
| CDR-SB | MMSE | ADAS-Cog13 | |
|---|---|---|---|
| Donanemab | −0.36 (−23%) | +0.64 (−21%) | −1.86 (−39%) |
| Aducanumab (high dose) | −0.39 (−22%); | +0.60 (−18%); | −1.40 (−27%); |
In early 2021, Eli Lilly thrilled about the success of clinical testing of donanemab. The current joy is much more restrained. The experimental therapy provided only modest control of cognitive and functional impairment, while not succeeding in slowing the progression of Alzheimer’s disease at least twice (the assumption on which the calculation of the statistical power of the clinical trial was based).
Again, the choice of the unusual primary endpoint stated by the iADRS composite score is remarkable: clinical trials in the context of Alzheimer’s disease usually address the CDR-SB scale — and on this score, donanemab failed to achieve a statistically significant difference with the control group. Therefore, it is appropriate to consider the array of other secondary endpoints to be purely exploratory, i.e., bearing no evidence of the clinical relevance of this drug candidate.
Administration of donanemab did not result in a drop in overall tau protein levels. Perhaps the lack of effect on tau load can be explained by the time lag when the 18-month observation period is too short for an appropriate response. Thus, models involving patients with autosomal dominant Alzheimer’s disease have provided insight into a delay of 10–20 years from the first PET detection of changes in amyloid beta levels to the first PET detection of changes in tau protein levels.
Much more paradoxical are the changes in the volume of the brain and its sections. In general, brain atrophy is typical in the natural course of Alzheimer’s disease but in the setting of donanemab it remains unclear whether the atrophy observed is the result of rapid structural removal of neurotoxic protein aggregates.
Be that as it may, Eli Lilly remains committed to further study of donanemab because all secondary endpoints achieved a statistically significant difference with the placebo group at least once in any of the time steps in the clinical trial.
Eli Lilly also pointed out the importance of selecting suitable patients: individuals with high levels of tau protein were excluded from participation in TRAILBLAZER-ALZ because their disease tends to progress more quickly. In fact, we are dealing with selection based on the pathological stage of Alzheimer’s disease — similar to the way patients are carefully selected for clinical trials of any cancer drugs.
Extras
Eli Lilly. Donanemab update. March 15, 2021. [PDF]
Donanemab in early Alzheimer’s disease. N Engl J Med. 2021 Mar 13. [source]
Donanemab slows progression of early symptomatic Alzheimer’s disease in phase 2 proof of concept trial. [PDF]
Donanemab (LY3002813) dose‐escalation study in Alzheimer’s disease. Alzheimers Dement (N Y). 2021; 7(1): e12112. [source]