Highlights
Auvelity (dextromethorphan + bupropion, 45 mg/105 mg) is a new oral drug indicated for the treatment of major depressive disorder (MDD) in adults.
Unlike all existing oral antidepressants, Auvelity, also known by the codename AXS-05, is characterized by rapid and prolonged therapeutic action. Improvement of depressive symptoms is noted literally in a week, remission comes in two. Auvelity can successfully manage the symptoms of even severe depression in most patients.
The medical need for new antidepressants that are effective and safe is extremely high due to the continued increase in the prevalence of depression worldwide.
Thus, in the U.S. alone, there were 21 million adults in 2020 who had experienced at least one episode of major depressive disorder in the previous year. Between March and April 2021, an estimated 85 million U.S. adults are facing elevated depressive symptoms, due in large part to the ongoing COVID-19 pandemic.
Auvelity was developed by Axsome Therapeutics.
The U.S. Food and Drug Administration (FDA) approved Auvelity in mid-August 2022.
Auvelity will go on sale in early fourth quarter of 2022. The price of Auvelity will be determined in the coming weeks.
Axsome is looking for a commercial partner to bring the drug to market outside the United States.
The U.S. regulator was supposed to decide on approval of Auvelity back in late August 2021. However, the FDA requested additional data from Axsome to resolve an incomplete New Drug Application (NDA) related to analytical methods in the Chemistry, Manufacturing, and Controls (CMC) section of the NDA. At that time, Axsome’s stock price lost nearly 40%, later recovering from the drop although not in full.
Axsome intends to expand Auvelity’s range of indications by confirming its utility in agitation therapy in Alzheimer’s disease and as an adjuvant in the treatment of nicotine addiction for those wishing to quit smoking.

What Is Major Depressive Disorder
Major depressive disorder (MDD), or clinical depression, is a chronic, disabling, biologically-based disorder characterized by depressed mood, inability to feel satisfaction, feelings of guilt and worthlessness, loss of energy, and other emotional and physical symptoms. In severe cases, the patient may resort to suicide. [1] [2]
Depression is a worldwide prevalent illness and one of the leading causes of disability. Approximately 3.8% of the world’s population is affected by depression, with 280 million people suffering from it. In low- and middle-income countries, the problem of depression is particularly acute: Factors such as lack of resources, lack of trained medical professionals, and social stigma associated with mental disorders are obstacles to effective treatment of depression. Misdiagnosis of people with depression is not uncommon in countries of all income levels. [3]
Major depressive disorder is difficult to treat: Nearly two-thirds of patients do not respond adequately to existing oral antidepressant first-line therapy. Most initial treatment failures also end in failure of all subsequent lines of therapy. [4]
Patients with clinical depression are diagnosed with treatment-resistant depression (TRD) if they do not respond to two or more lines of therapy with antidepressants of different pharmacological classes.
Currently approved oral antidepressants act primarily through monoaminergic mechanisms. Since achieving a clinically significant response requires a long time of their continuous use (up to 6–8 weeks), and the therapy itself is accompanied by adverse events, it seriously affects the patients’ adherence to treatment, often they prematurely discontinue therapy. [4] [5] [6]
That is why there is a high unmet medical need for fundamentally new pharmacotherapeutic options for the treatment of major depressive disorder. Such drugs must be well tolerated, act quickly, and provide a sustained clinical effect. [7]
Auvelity: Combined Mechanism of Action of Dextromethorphan With Bupropion
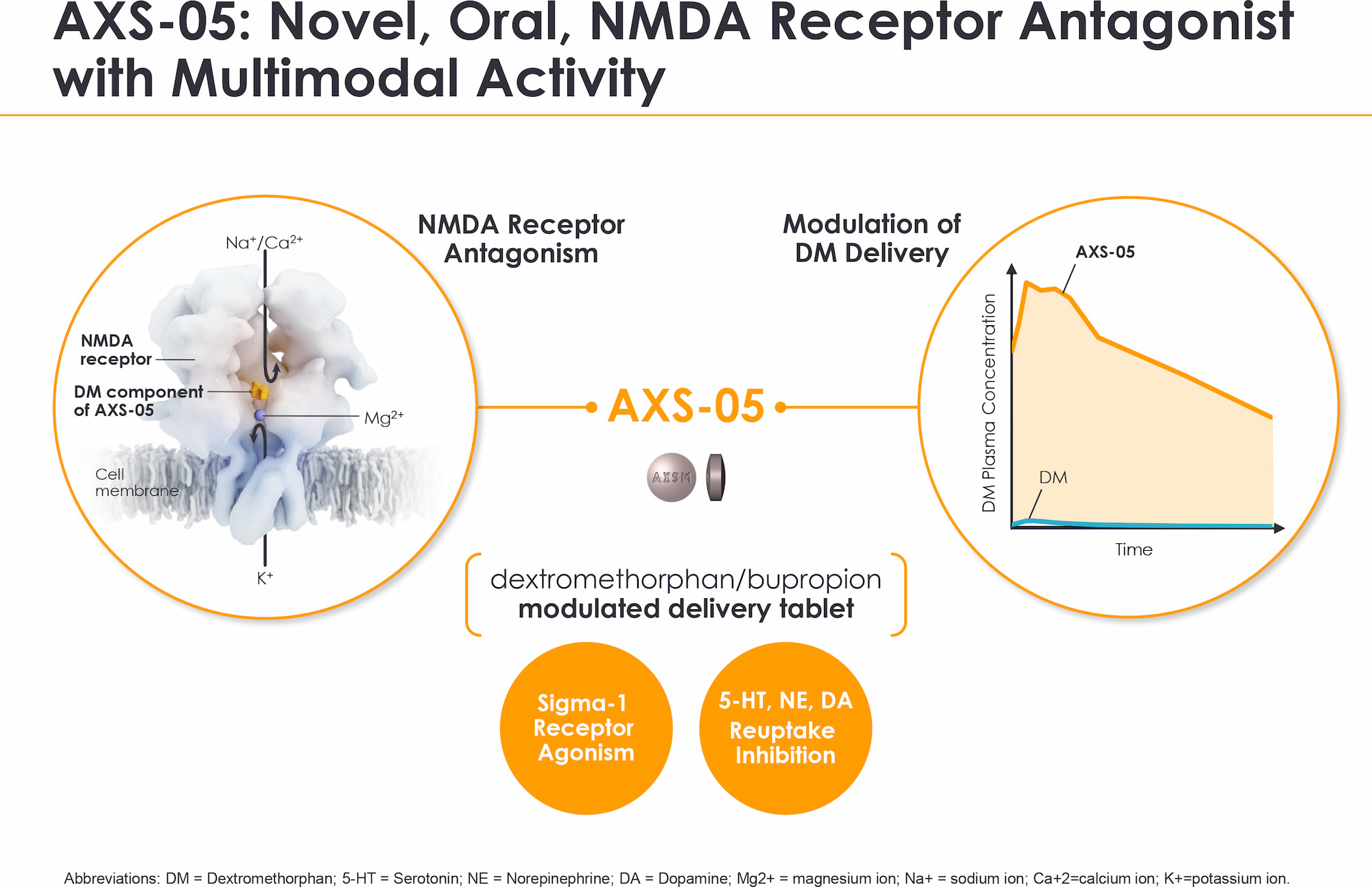
The combined oral drug Auvelity (dextromethorphan + bupropion, 45 mg/105 mg), known by the codename AXS-05, is an N-methyl-D-aspartate (NMDA) receptor antagonist with multimodal activity.
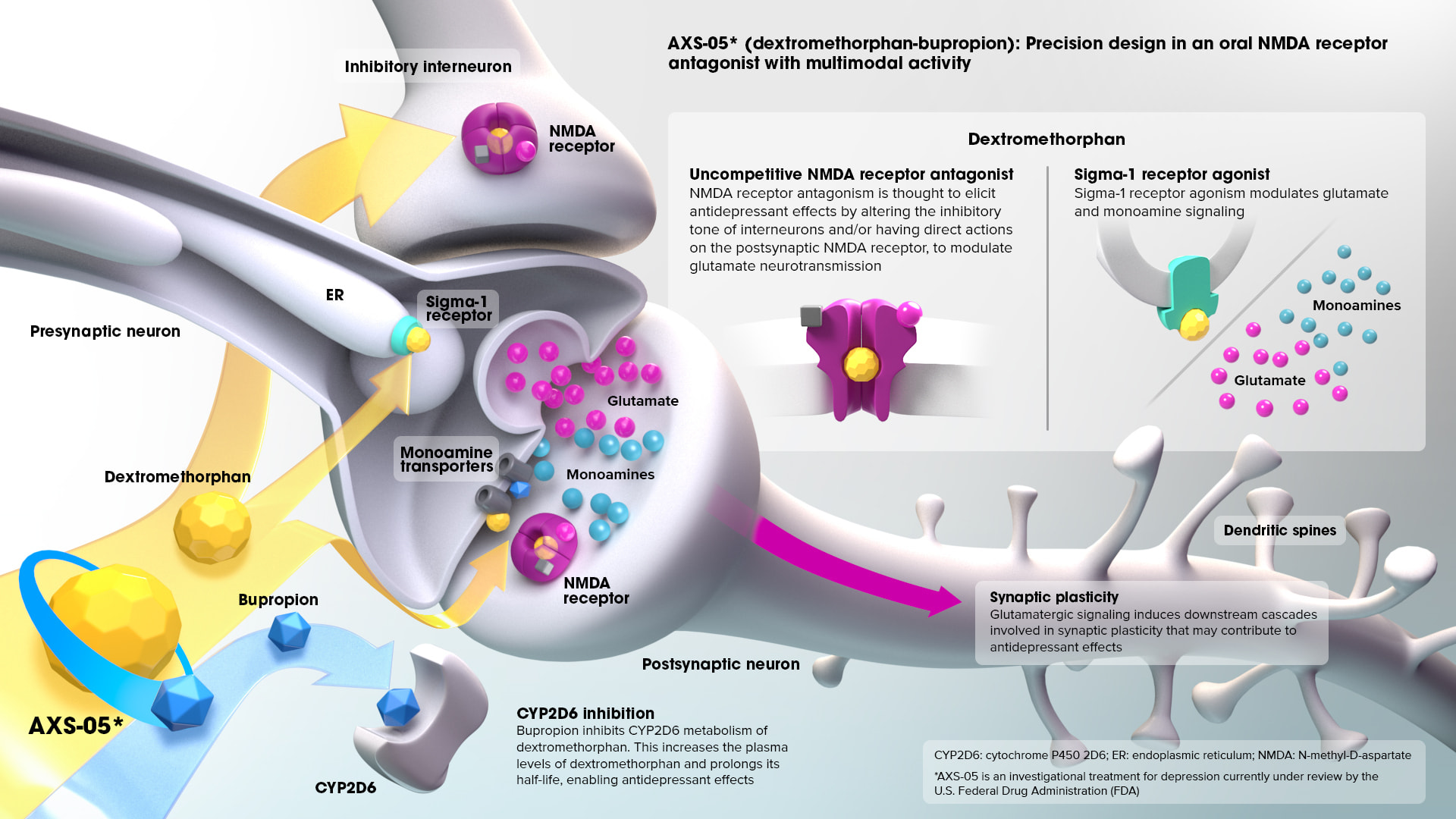
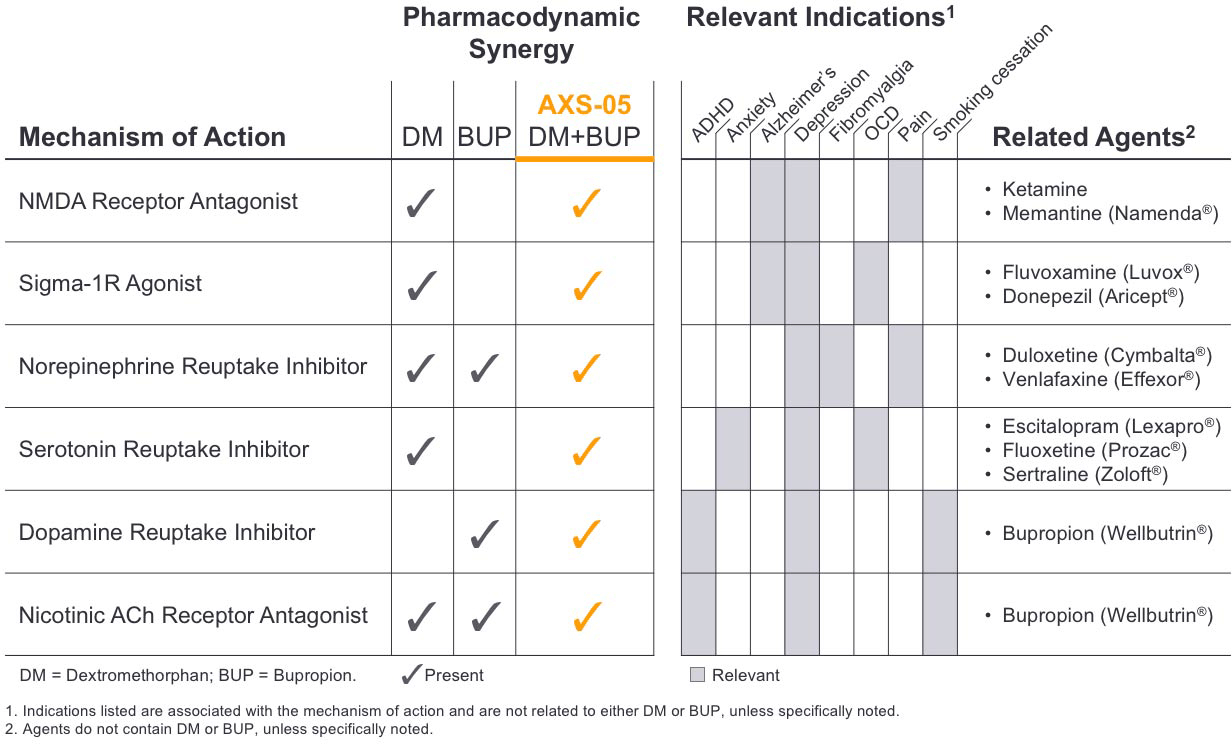
Dextromethorphan, being a non-competitive NMDA receptor antagonist, also works as a sigma-1 receptor agonist and inhibitor of serotonin and noradrenaline transport proteins.
Antagonism of the NMDA receptor, which is an ionotropic glutamate receptor, causes an antidepressant effect realized by modulation of glutamate neurotransmission by changing the inhibitory tone of interneurons and/or direct action on the postsynaptic NMDA receptor. Agonism of sigma-1 receptor modulates glutamate and monoamine signaling. [1]
- It is well known that NMDA receptor antagonism with ketamine leads to rapid and significant antidepressant effects. [2] However, the use of ketamine comes with a number of challenges, including parenteral administration, potential for abuse, psychotomimetic side effects, and a narrow therapeutic window. Nevertheless, in March 2019, Janssen of Johnson & Johnson succeeded in bringing Spravato (esketamine) to market for treatment-resistant depression and then, in August 2020, this nasal spray added treatment for major depressive disorder with acute suicidal ideation and behavior. Esketamine is the S(+)-enantiomer of ketamine.
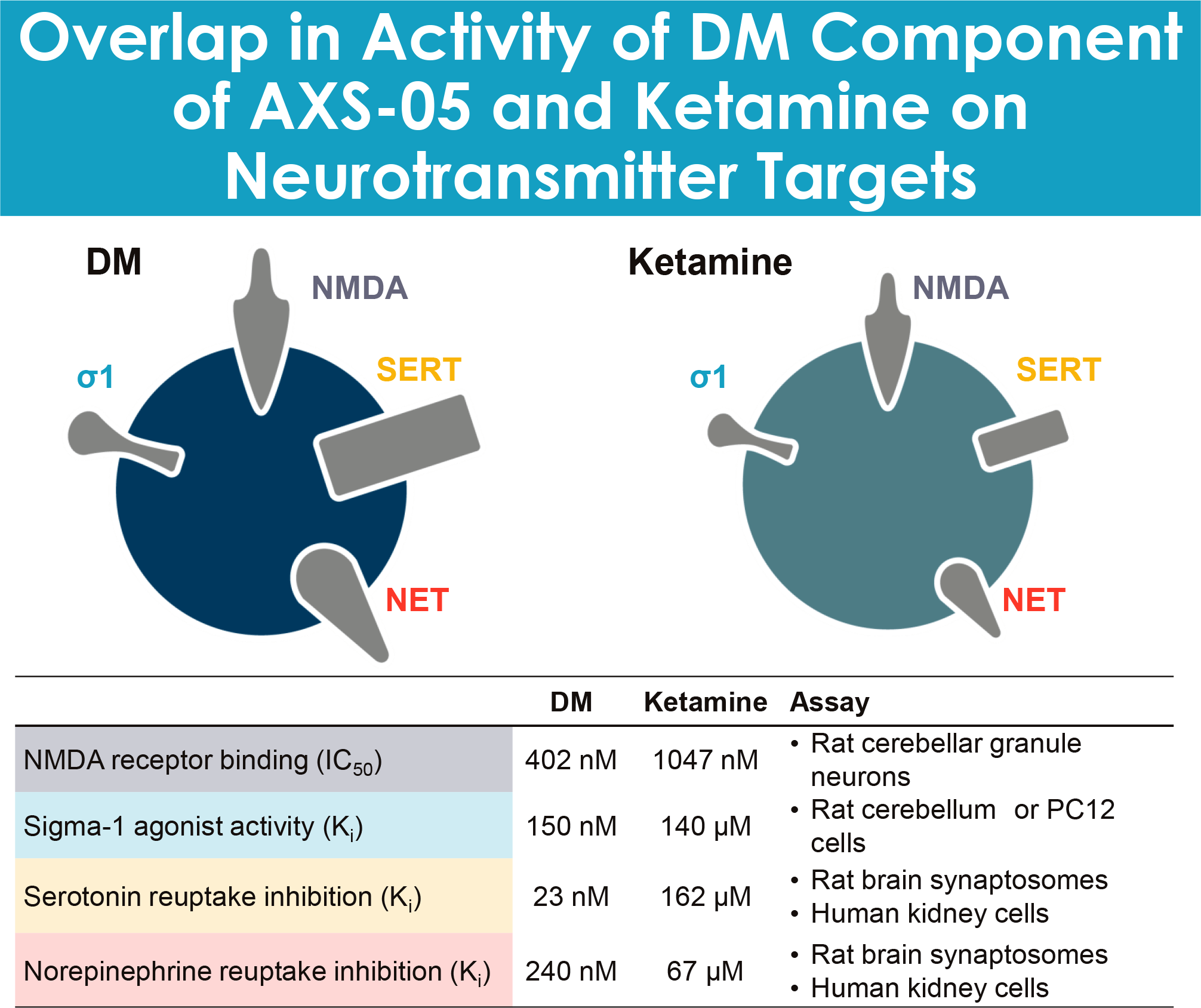
- The similarities between dextromethorphan and ketamine in terms of receptor pharmacology and pharmacodynamic effects suggest that dextromethorphan has antidepressant efficacy without the limitations of ketamine. However, whether the antidepressant effect is due specifically to NMDA receptor antagonism is still unclear. [3] [4]
Bupropion serves as a bioavailability enhancer for dextromethorphan, which is metabolized too quickly in the human body, not reaching the plasma concentrations necessary to achieve the desired psychotherapeutic effects. Bupropion inhibits cytochrome P450 2D6 (CYP2D6)-mediated dextromethorphan metabolism, which is reflected by increased dextromethorphan plasma levels and prolongation of its half-life. Thus, the antidepressant effect is sustained. [5]
Bupropion also acts as an inhibitor of norepinephrine and dopamine reuptake. [6]
In addition, dextromethorphan and bupropion are nicotinic acetylcholine receptor antagonists.
The complex antidepressant mechanism of action of Auvelity is tied to a number of signaling cascades relevant to synaptic plasticity, and is provided by strengthening synaptic connections and improving communication interactions between brain cells. The drug compound increases brain levels of serotonin, norepinephrine and dopamine, which are key neurotransmitters involved in mood regulation.
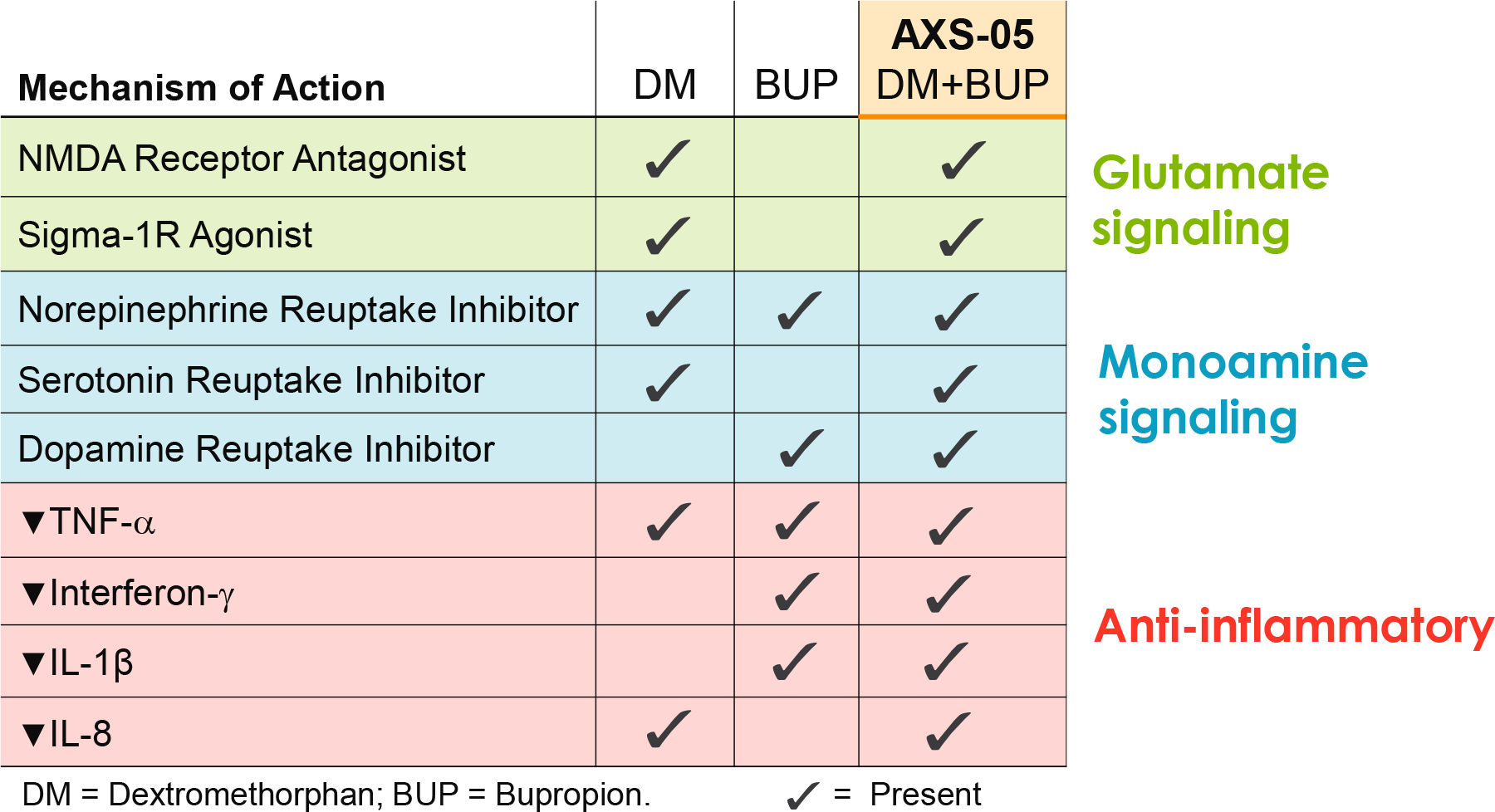
Auvelity has also been noted to have anti-inflammatory properties. [7] [8] [9] [10] [11] There is a link between depression and inflammation: patients with depression have elevated serum levels of interleukin 6 (IL-6), interleukin 1 (IL-1), C-reactive protein (CRP), tumor necrosis factor (TNF) and other inflammatory biomarkers. [12] [13] [14] [15] [16]
Auvelity: Efficacy and Safety of Treating Major Depressive Disorder
Main Study
The GEMINI (NCT04019704) phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled adult patients (n=327) with moderate-to-severe (total MADRS score ≥ 25) major depressive disorder.
Subjects’ baseline characteristics were as follows: mean age 42 years, 66% female, mean MADRS total score 33.
Patients received twice-daily placebo or dextromethorphan with buprion for 6 weeks; participants received only one dose on the first three days.
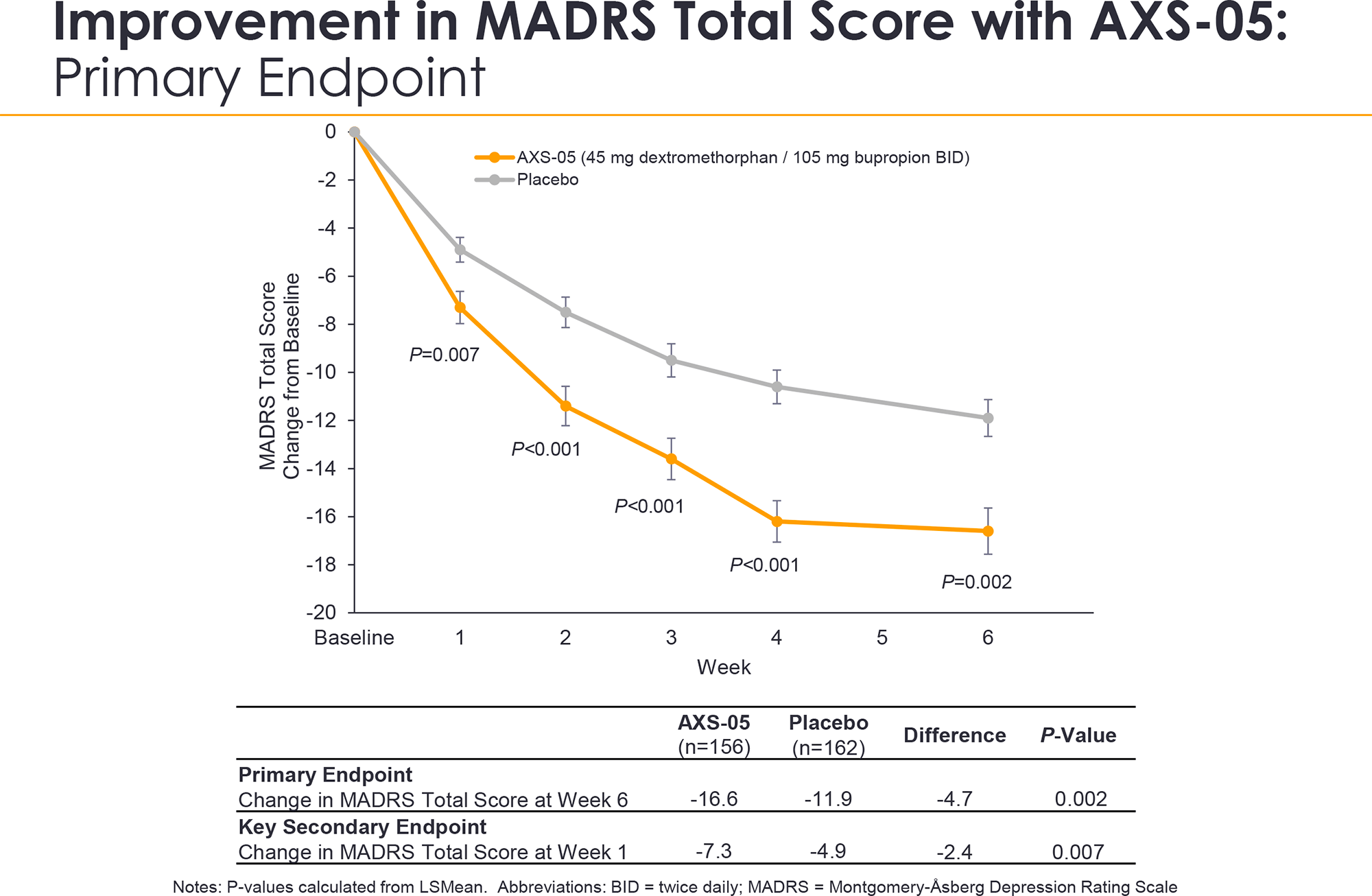
The primary efficacy endpoint of therapy was stated to be the change in the Montgomery–Åsberg Depression Rating Scale (MADRS) total score after 6 weeks (higher score — more severe depression].
The Auvelity group showed a decrease in MADRS total score by a mean of 16.6 points — versus 11.9 points in the placebo group (p=0.002).
Those receiving dextromethorphan with buprion showed a statistically significant (p=0.007) difference with the control group as early as week 1 of treatment: the MADRS total score decreased by a mean of 7.3 points — versus 4.9 points.
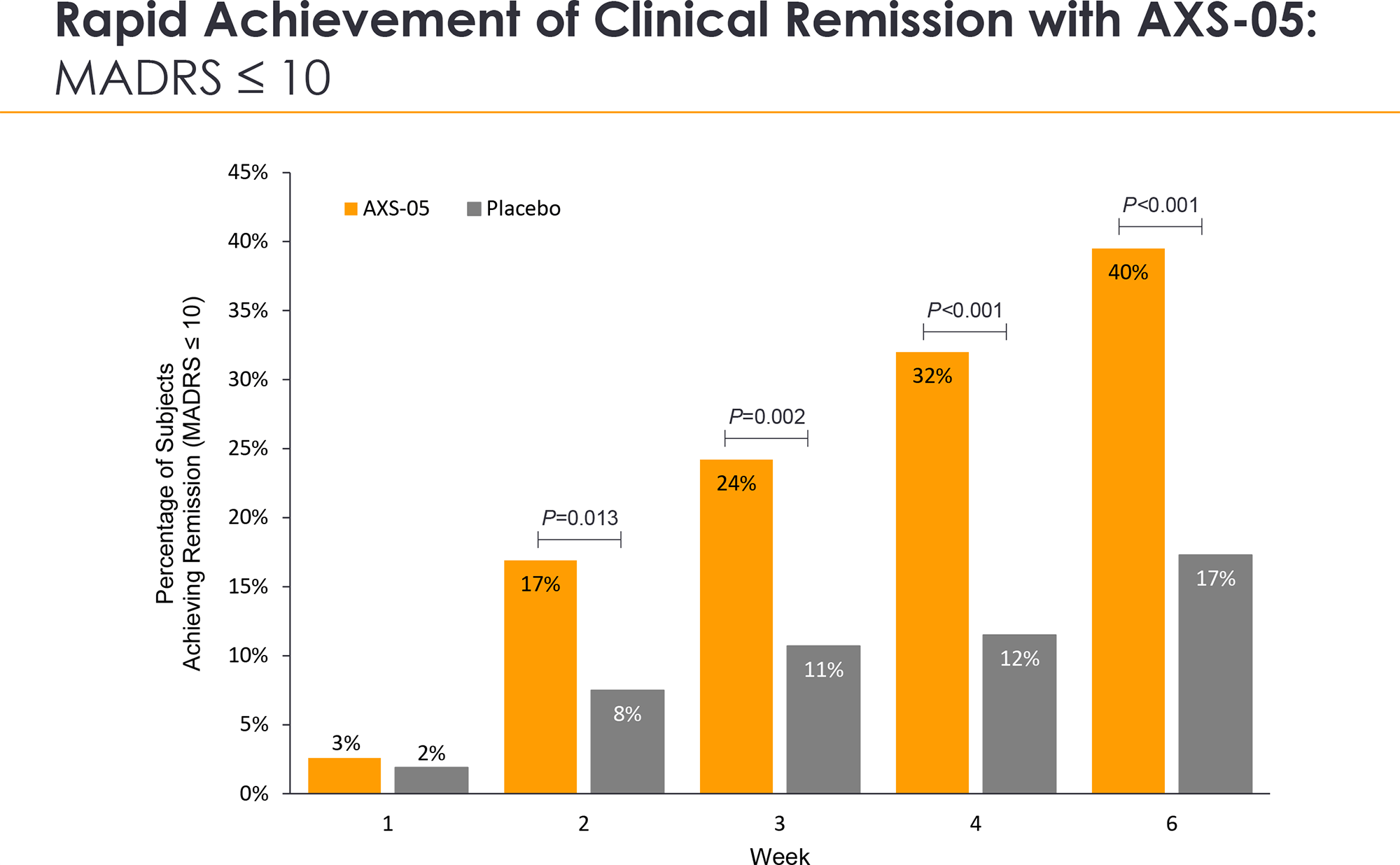
Administration of Auvelity resulted in clinical remission (absence of clinically significant symptoms of depression and MADRS total score ≤ 10) after 2, 3, 4, and 6 weeks of therapy in 17%, 24%, 32%, and 40% of patients — vs. 8%, 11%, 12%, and 17% in the placebo group (p=0.013, p=0.002, p<0.001, p<0.001).
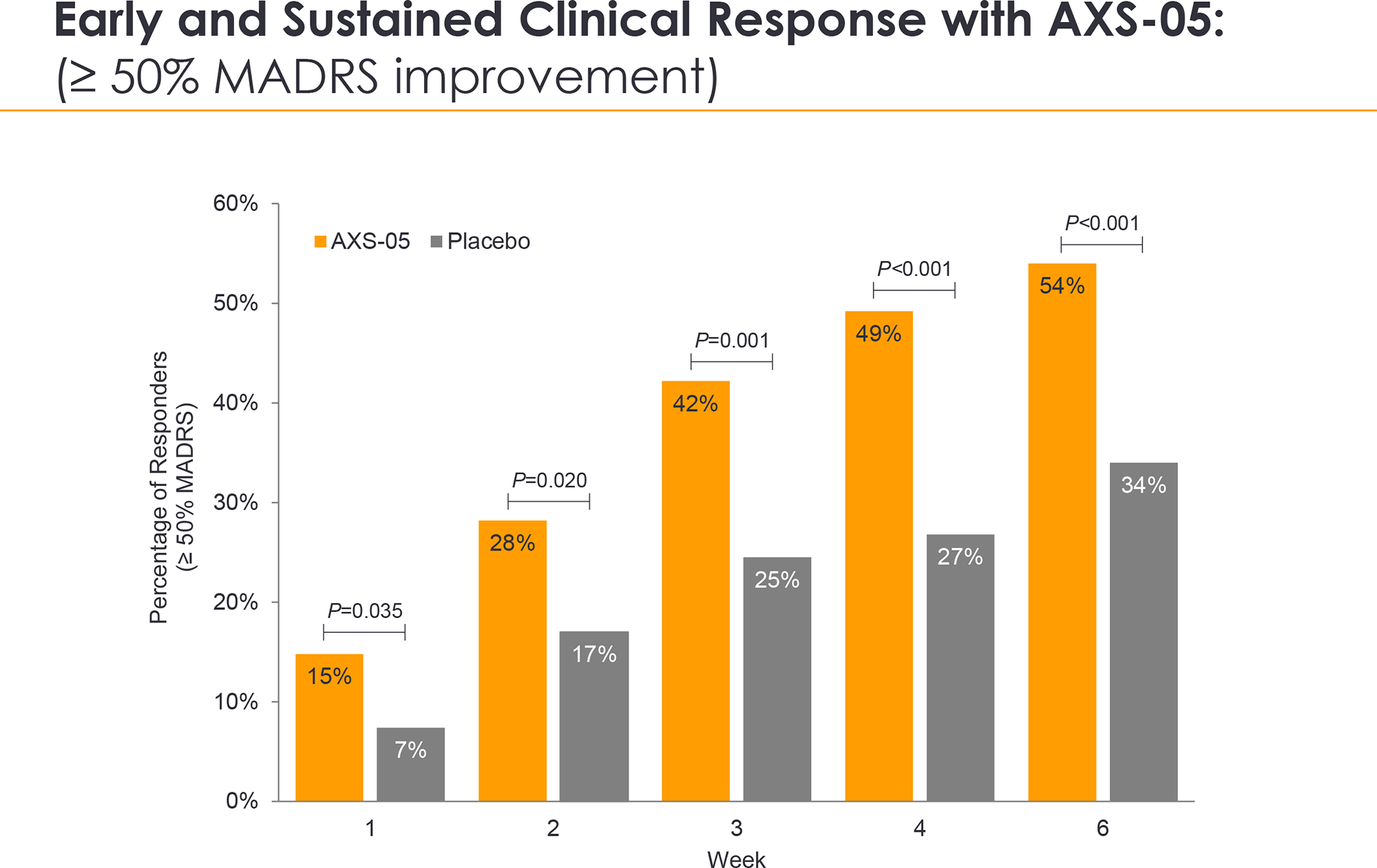
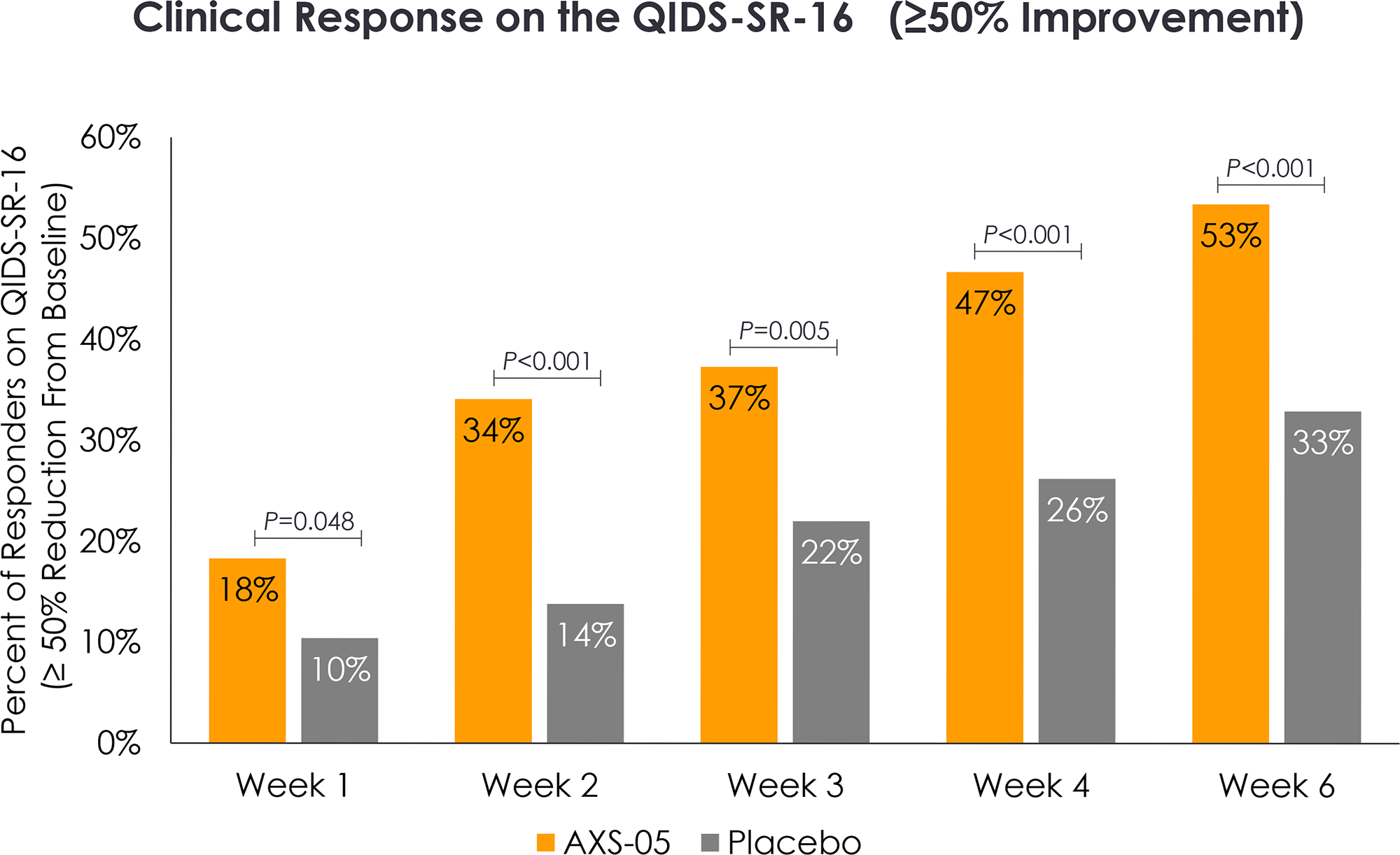
Auvelity treatment led to an early and sustained clinical response (≥ 50% reduction in the MADRS total score) after 1, 2, 3, 4, and 6 weeks of treatment in 15%, 28%, 42%, 49%, and 54% of patients — vs. 7%, 17%, 25%, 27%, and 34% in the placebo group (p=0.035, p=0.020, p=0.001, p<0.001, p<0.001).
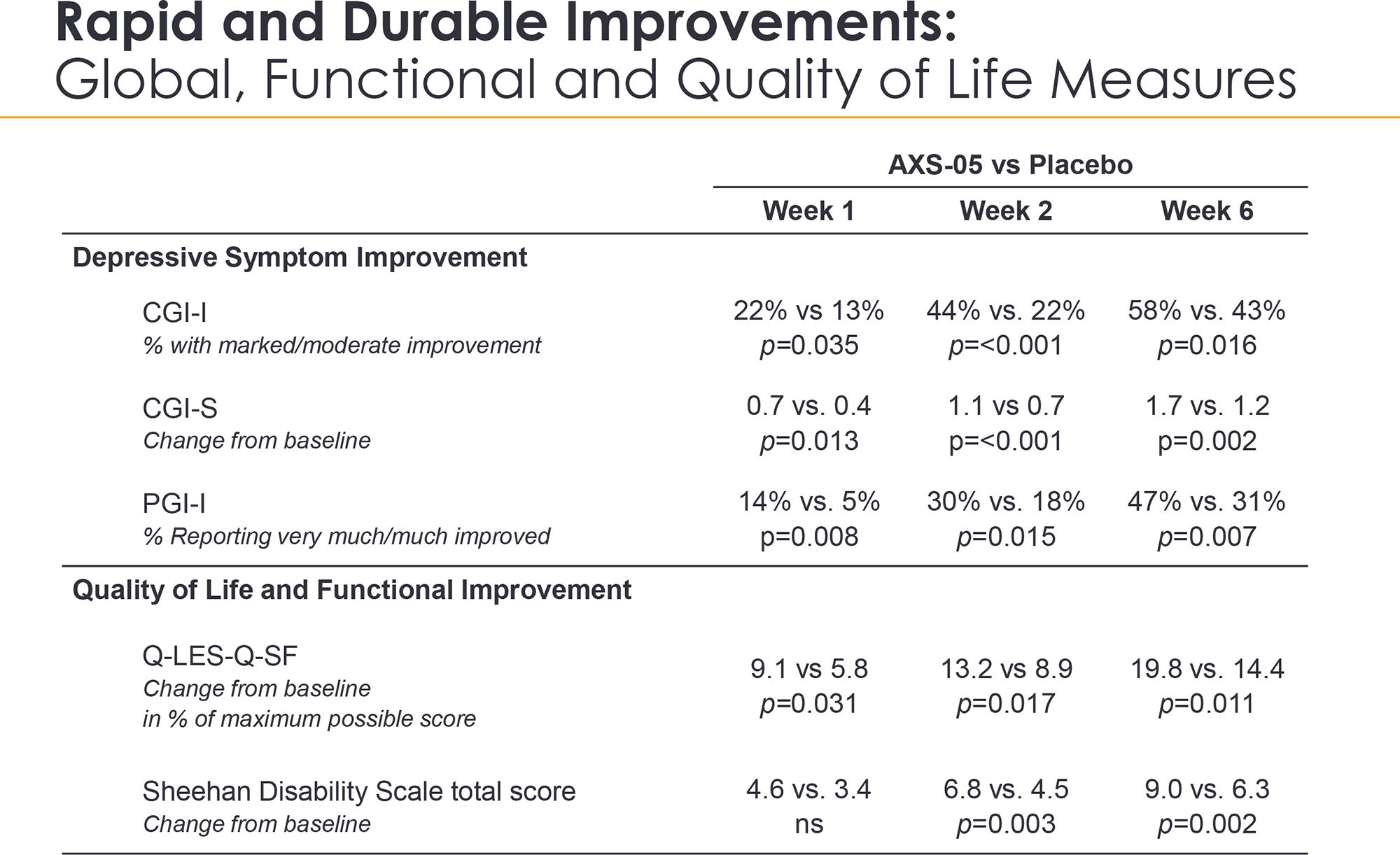
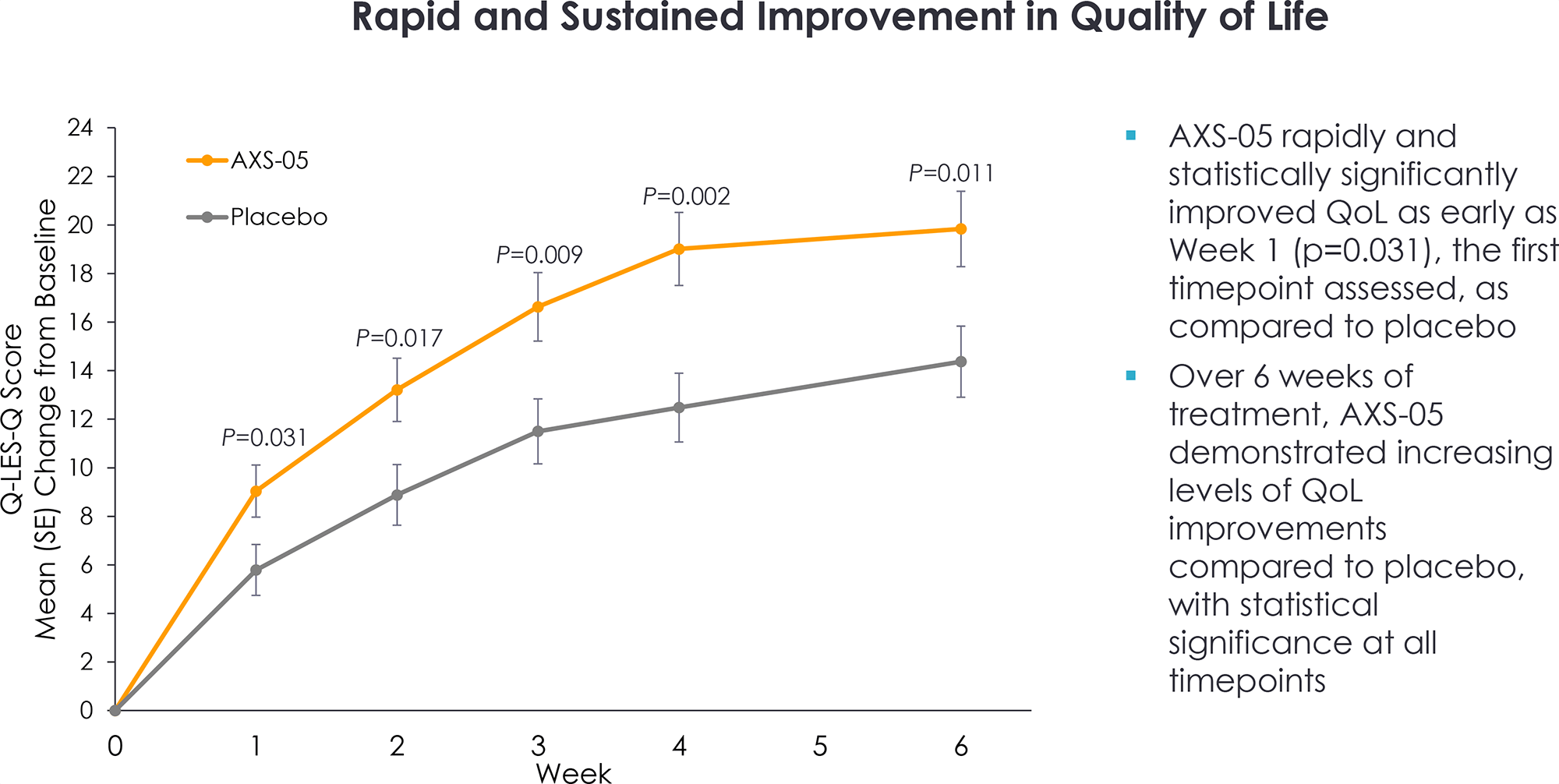
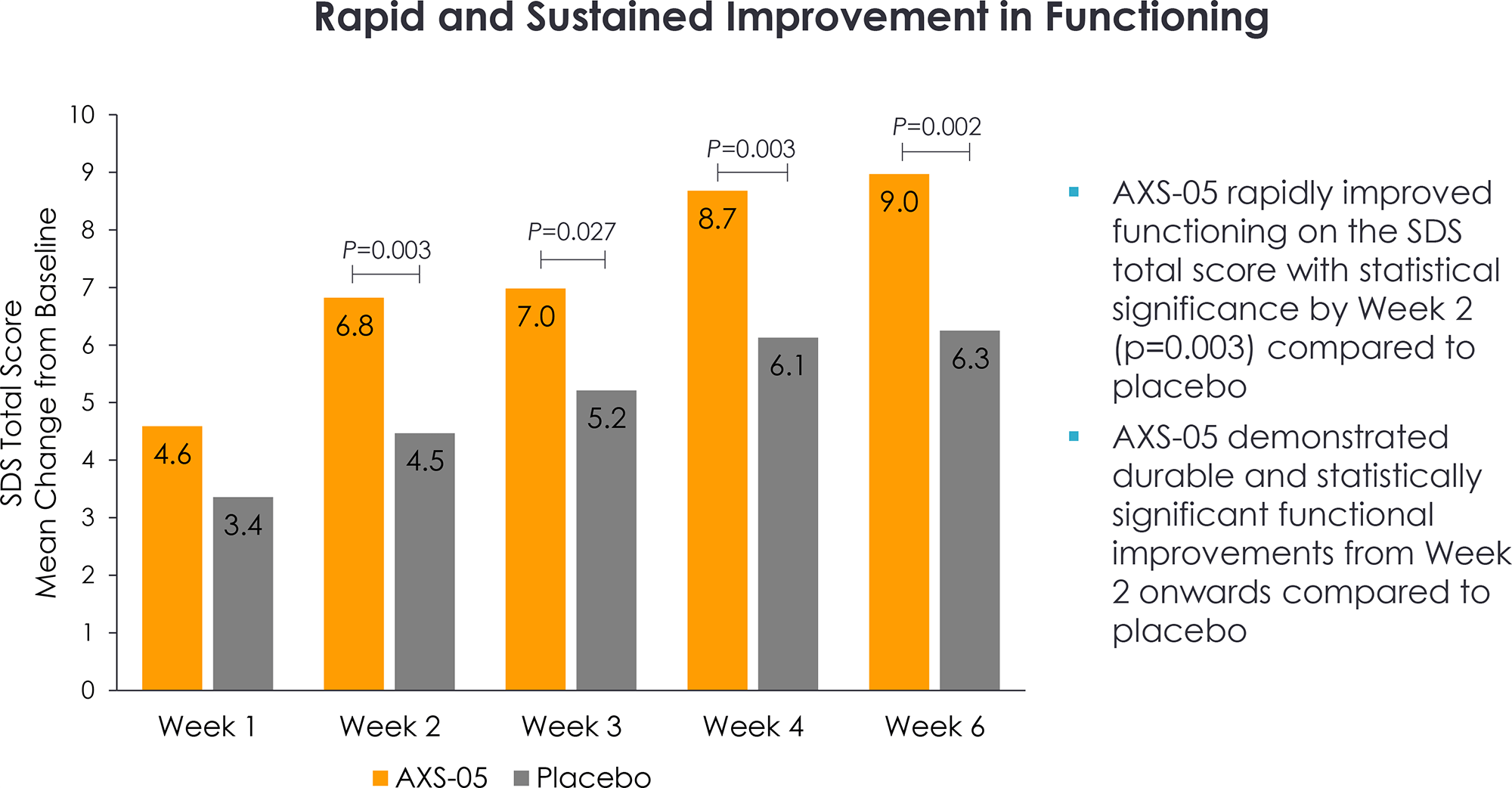
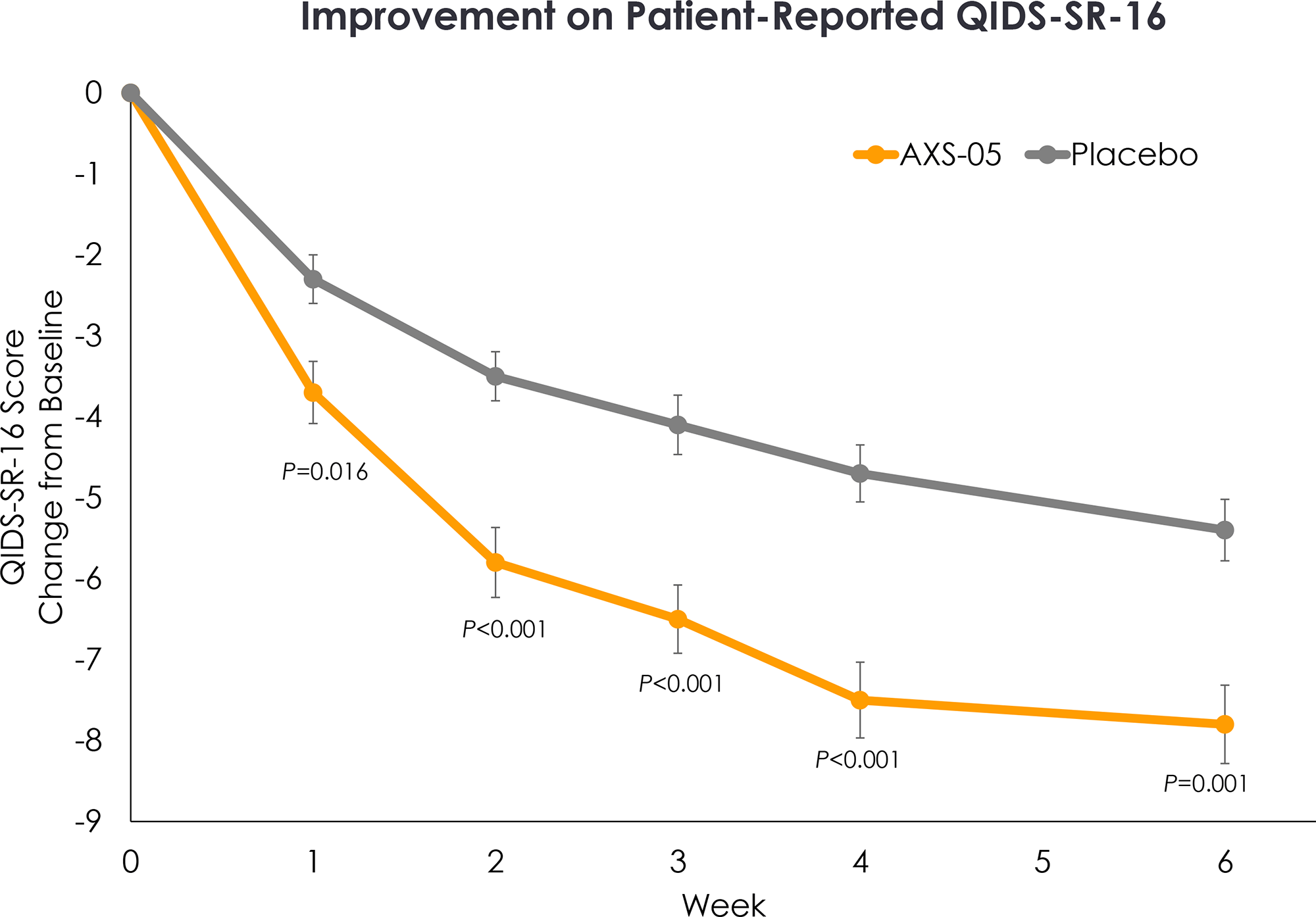
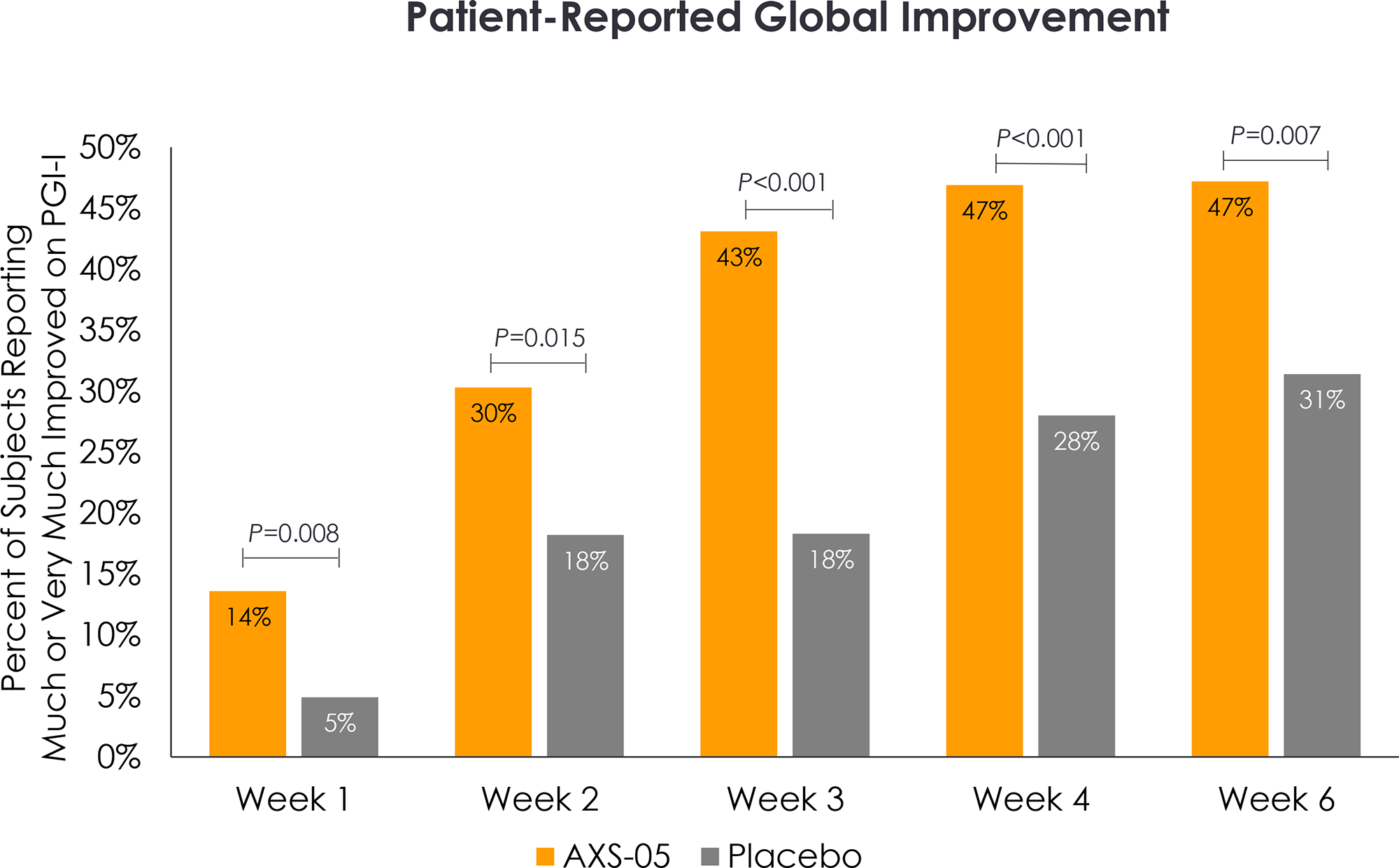
The combination of dextromethorphan and buprion had statistically significant effects on improving scores on the Clinical Global Impression–Improvement scale (CGI-I), the Clinical Global Impression–Severity scale (CGI-S), the Patient Global Impression–Improvement scale (PGI-I), the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-SF), the Quick Inventory of Depressive Symptomatology–Self-Report (QIDS-SR-16).
The safety profile of Auvelity was characterized by acceptable tolerability. The most common adverse events included dizziness (in 16% of patients in the Auvelity group — versus 6% in the placebo group), nausea (13% vs. 9%), headache (8% vs. 4%), diarrhea (7% vs. 3%), somnolence (7% vs. 3%), and dry mouth (6% vs. 2%). All adverse reactions were mild-to-moderate in severity.
The prescribing information for Auvelity is given with a boxed warning about the increased risk of suicidal thoughts and behavior in children, adolescents, and young adults (18-24 years) taking antidepressants. This patient population should be closely monitored for worsening clinical presentation and suicidal tendencies. Auvelity is not approved for use in pediatric patients.
Long-Term Study #1
The COMET (NCT04039022) phase 3 (nonrandomized, open-label, multicenter) clinical trial invited adult patients (n=611) with moderate-to-severe (total MADRS score ≥ 25) major depressive disorder.
Subjects’ baseline characteristics were as follows: mean age 42 years, 62% female, mean MADRS total score 33.
For 12 months, patients were administered twice daily dextromethorphan with buprion.
Long-term treatment of major depressive disorder with Auvelity resulted in the following therapy efficacy rates.
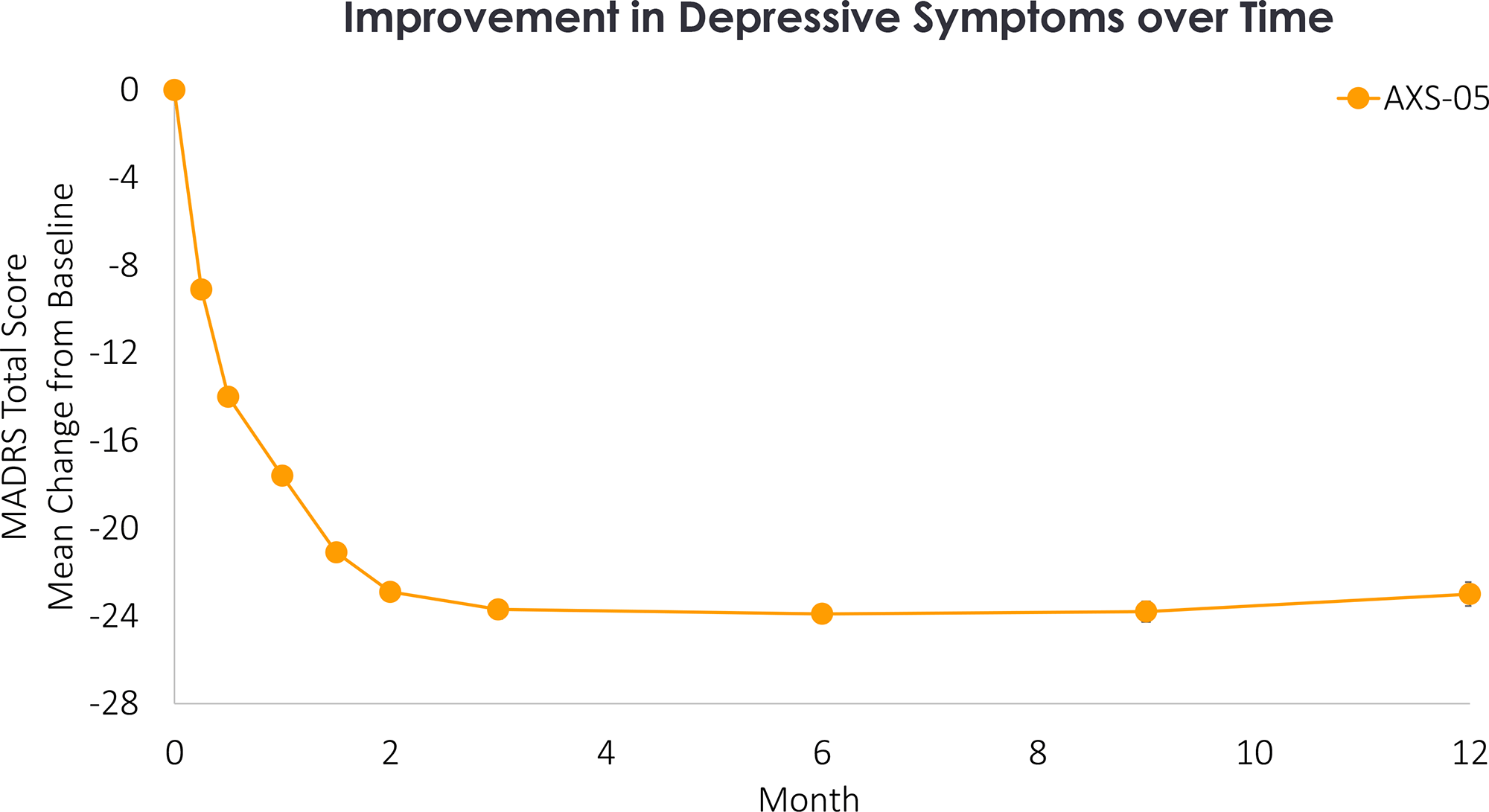
The mean decrease in the MADRS total score was 9.1, 14.0, and 21.1 points after 1, 2, and 6 weeks. After 6 and 12 months, this score decreased by 23.9 and 23.0 points.
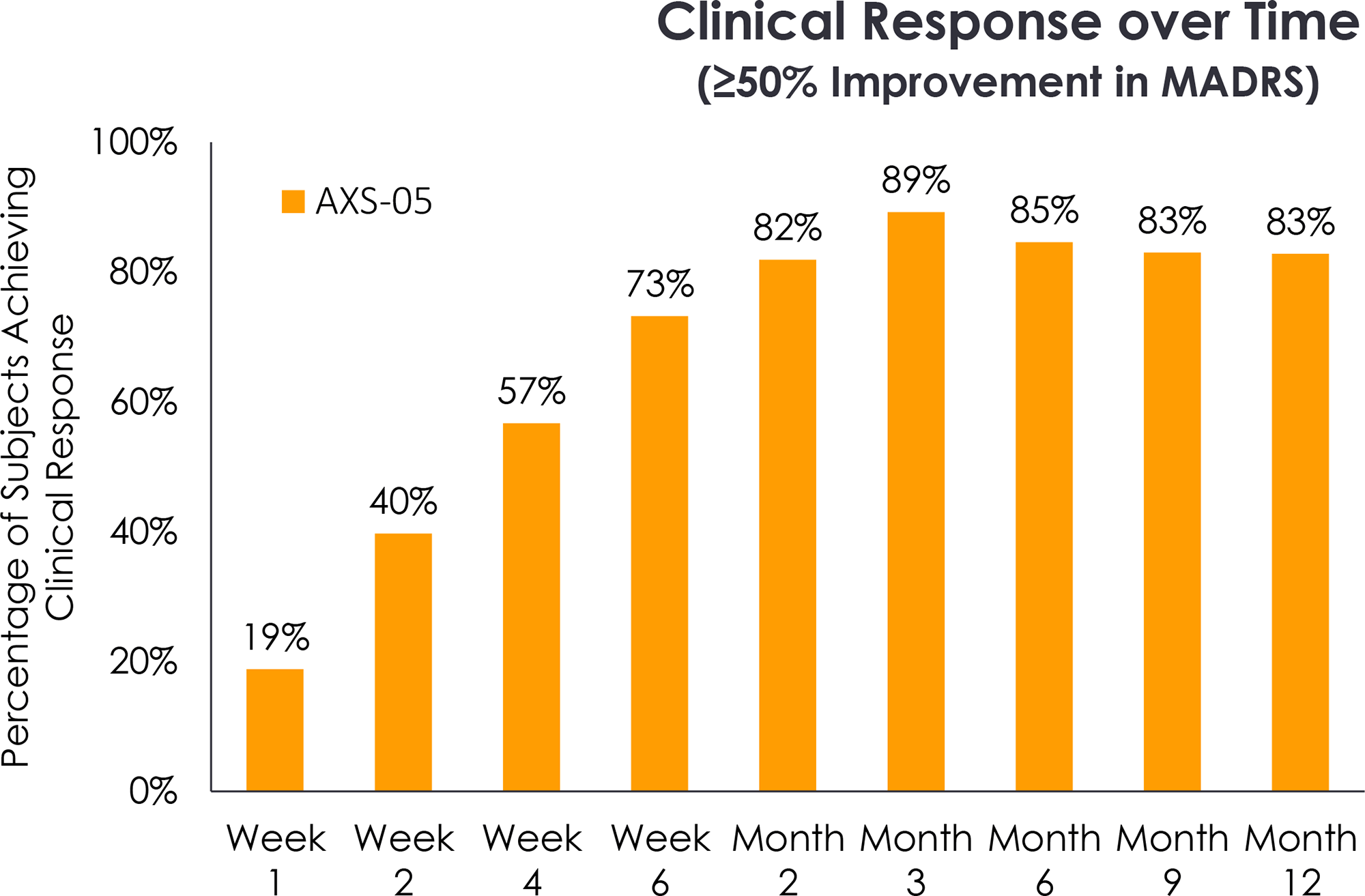
The clinical response status for depression treatment was 19%, 40%, and 73% of patients after 1, 2, and 6 weeks of therapy. Clinical response was fair for 85% and 83% of subjects after 6 and 12 months of treatment.
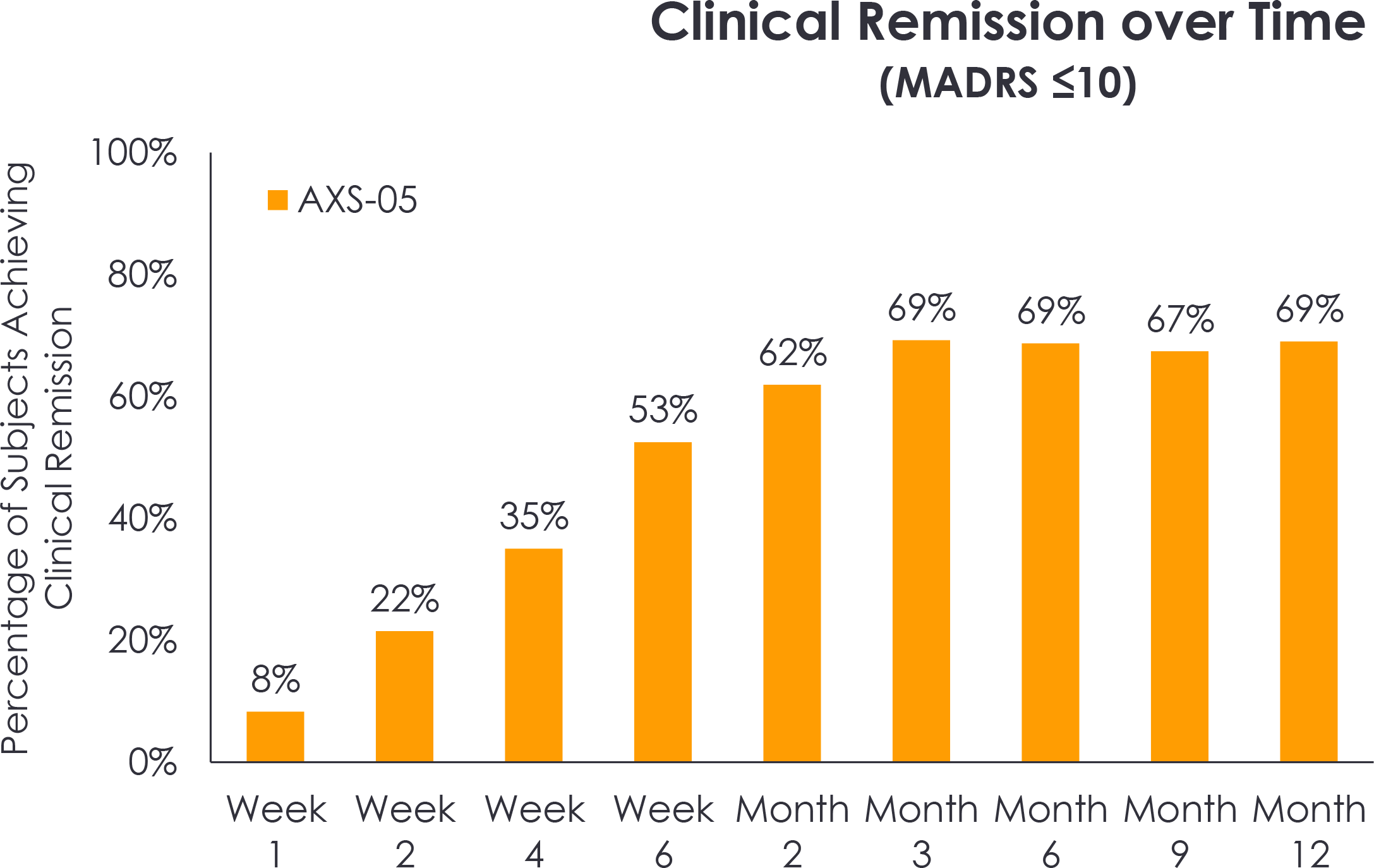
Clinical remission of depression was recorded for 8%, 22%, and 53% of patients after 1, 2, and 6 weeks of treatment. 69% and 69% of participants reached this status after 6 and 12 months of therapy.
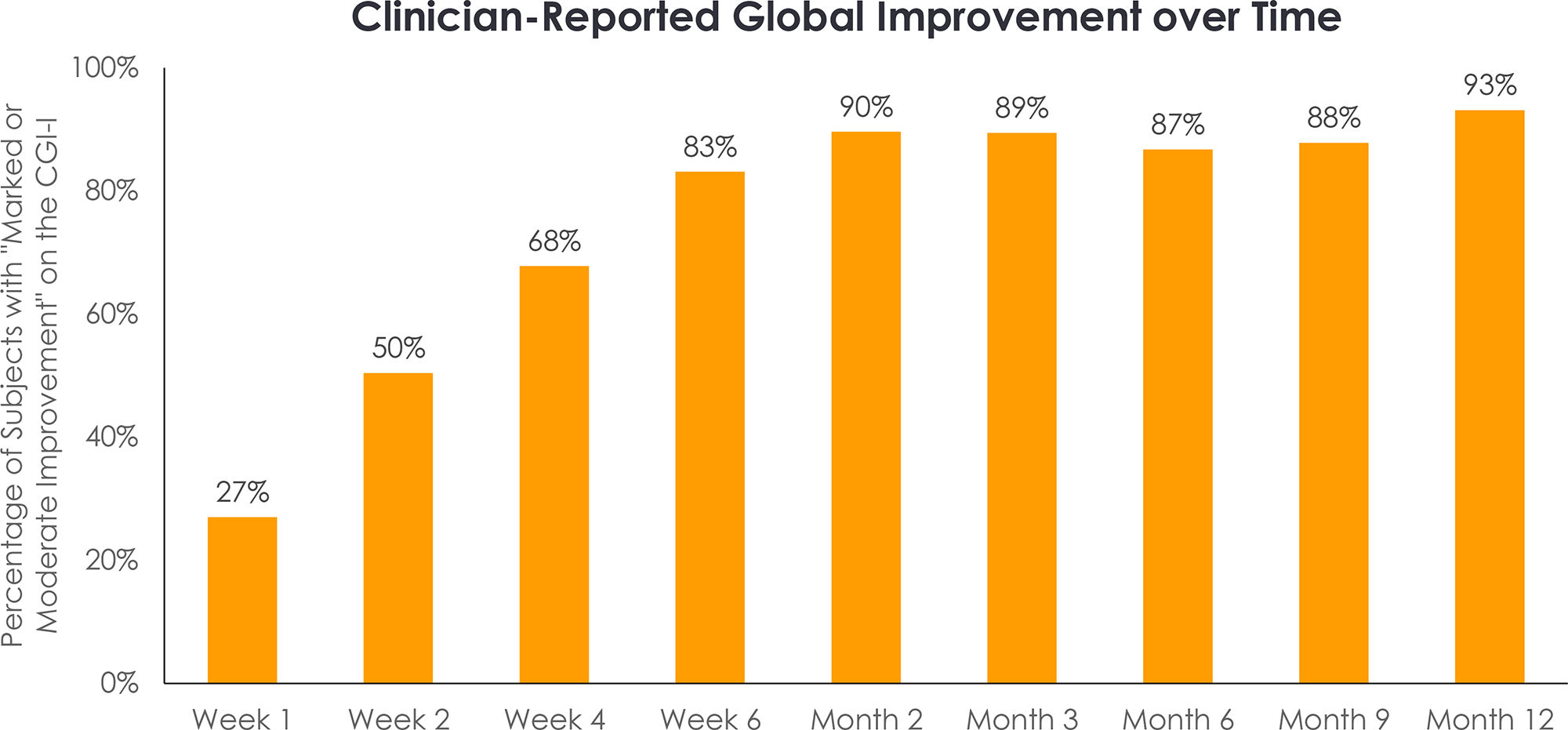
Clear improvements in depressive symptoms, as assessed by the CGI-I scale, were reported in 27%, 50%, and 83% of patients after 1, 2, and 6 weeks of treatment. The same was reported for 87% and 93% of patients after 6 and 12 months of therapy.
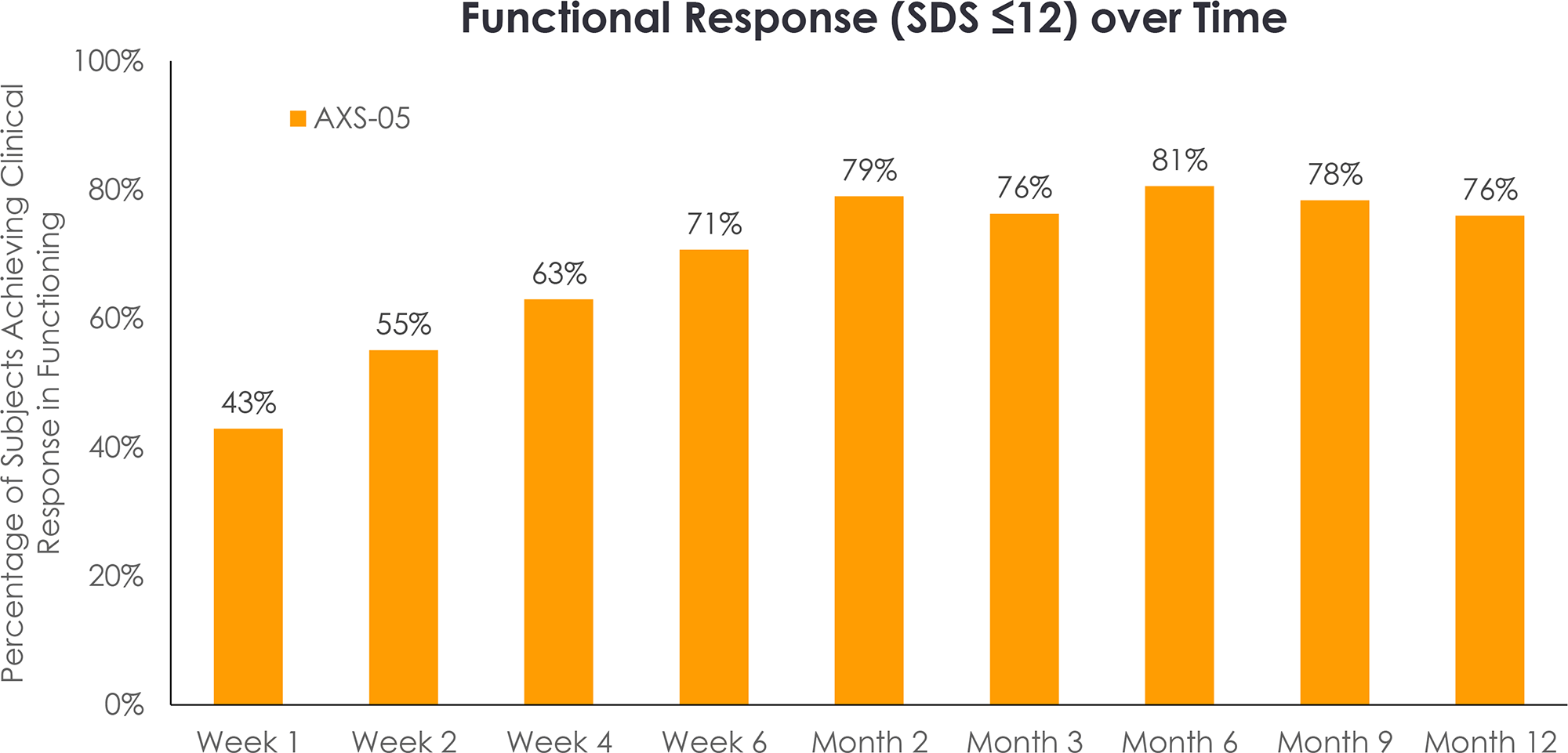
Clinical response (total score ≤ 12) to treatment of depression on the Sheehan Disability Scale (SDS), which assesses functional capacity in work/study, social life, and family life/household responsibilities, was evidenced for 42.9%, 55.1%, and 70.7% of patients after 1, 2, and 6 weeks of treatment. This was true for 81% and 76% of subjects after 6 and 12 months of therapy.
The safety profile of Auvelity was characterized by acceptable tolerability. The most common adverse events included dizziness (13% of patients), nausea (12%), headache (9%), dry mouth (7%), decreased appetite (6%). All adverse reactions were mild-to-moderate in severity.
Long-Term Study #2
The EVOLVE clinical trial (nonrandomized, open-label, multicenter) included adult patients (n=186) with moderate-to-severe (MADRS total score ≥25) major depressive disorder who had previously been treated with at least one antidepressant during a current episode of depression and whose treatment failed.
Baseline characteristics of the subjects: mean MADRS total score was 32.
Patients were given twice-daily dextromethorphan with buprion for up to 15 months.
Administration of Auvelity resulted in rapid improvement of depressive symptoms. Thus, the mean reductions in MADRS total score were 9.1±7.6 (p<0.001), 13.3±8.6 (p<0.001), and 20.4±7.8 (p<0.001) after 1, 2, and 6 weeks, respectively. Clinical response was reported for 17.7%, 39.0%, and 74.2% of patients. 5.7%, 16.2%, and 46.0% of subjects went into remission of major depressive disorder.
The antidepressant effect of Auvelity was characterized by durability and sustainability throughout the 12 months of therapy. Thus, remission status was fair for 65% and 68% of patients after 6 and 12 months of treatment.
Functional remission of major depressive disorder, according to the Sheehan Disability Scale (SDS; total score ≤ 6), was achieved by 18%, 31%, and 40% of patients after 1, 2, and 6 weeks of treatment. After 6 and 12 months of therapy, 54% and 59% of subjects reached the status of functional remission.
Administration of Auvelity provided relief of anxiety, according to the Hamilton Anxiety Rating Scale (HAM-A), in 36%, 51% and 58% of patients who achieved remission for this clinical indicator (total score ≤ 7) after 1, 2 and 6 weeks of treatment. Remission after 6 and 12 months of therapy was recorded for 75% and 78% of subjects.
Long-term administration of Auvelity was characterized by acceptable tolerability. The most common adverse events included nausea (in 8.9% of patients), headache (7.5%), dry mouth (6.2%), insomnia (5.5%), and dizziness (5.5%).
Additional Study
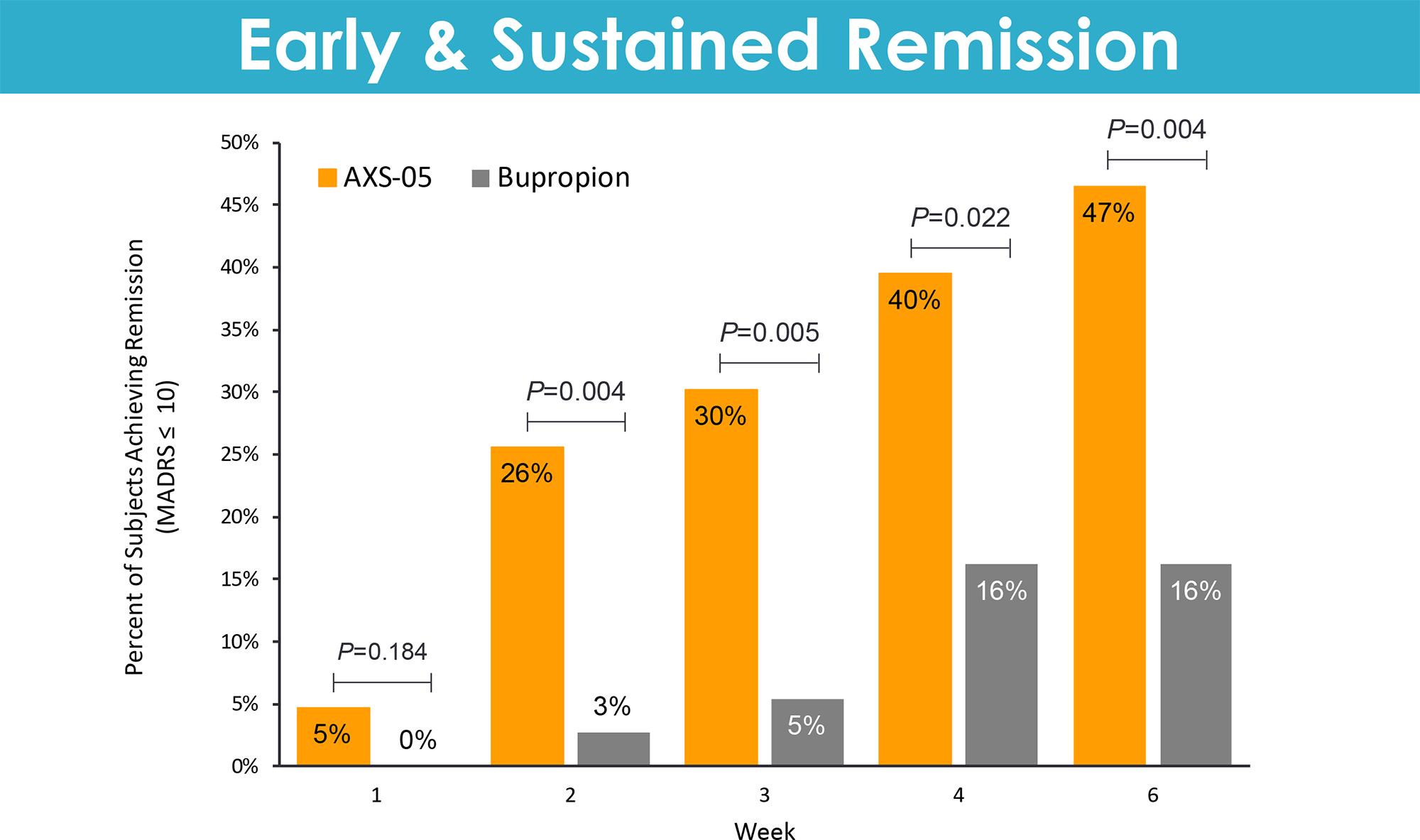
The ASCEND (NCT03595579) phase 2 (randomized, double-blind, active-controlled, multicenter) clinical trial enrolled adult patients (n=80) with moderate-to-severe (total MADRS score ≥25) major depressive disorder.
Subjects’ baseline characteristics were as follows: mean age 37,5 years, 64% female, mean MADRS total score 32.
Participants were given either dextromethorphan with bupropion or bupropion alone, twice daily for 6 weeks.
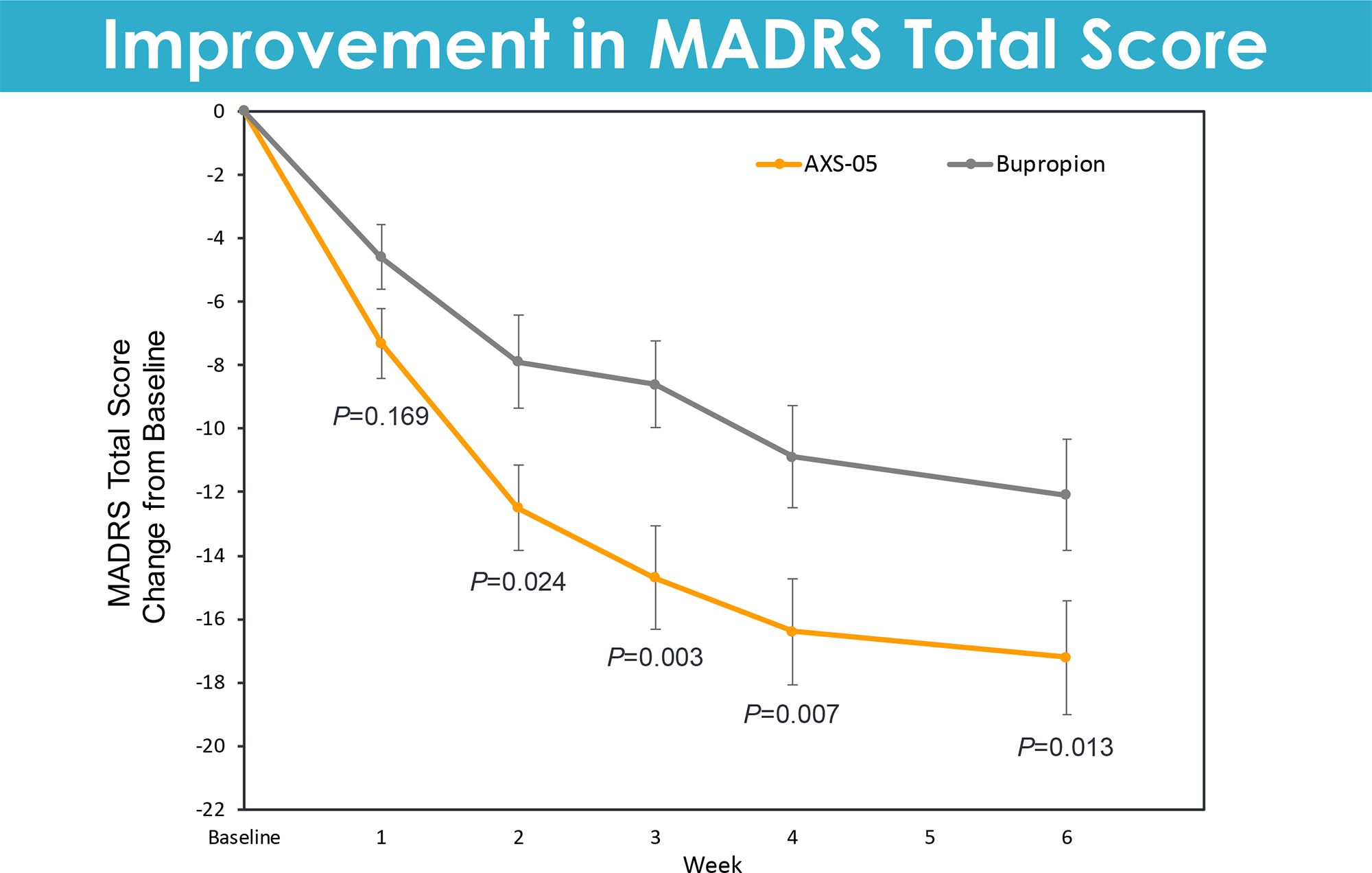
Auvelity provided a statistically significant reduction in total MADRS score: over the entire course of treatment, the reduction was a mean of 13.7 points — versus 8.8 points in the bupropion group (p<0.001).
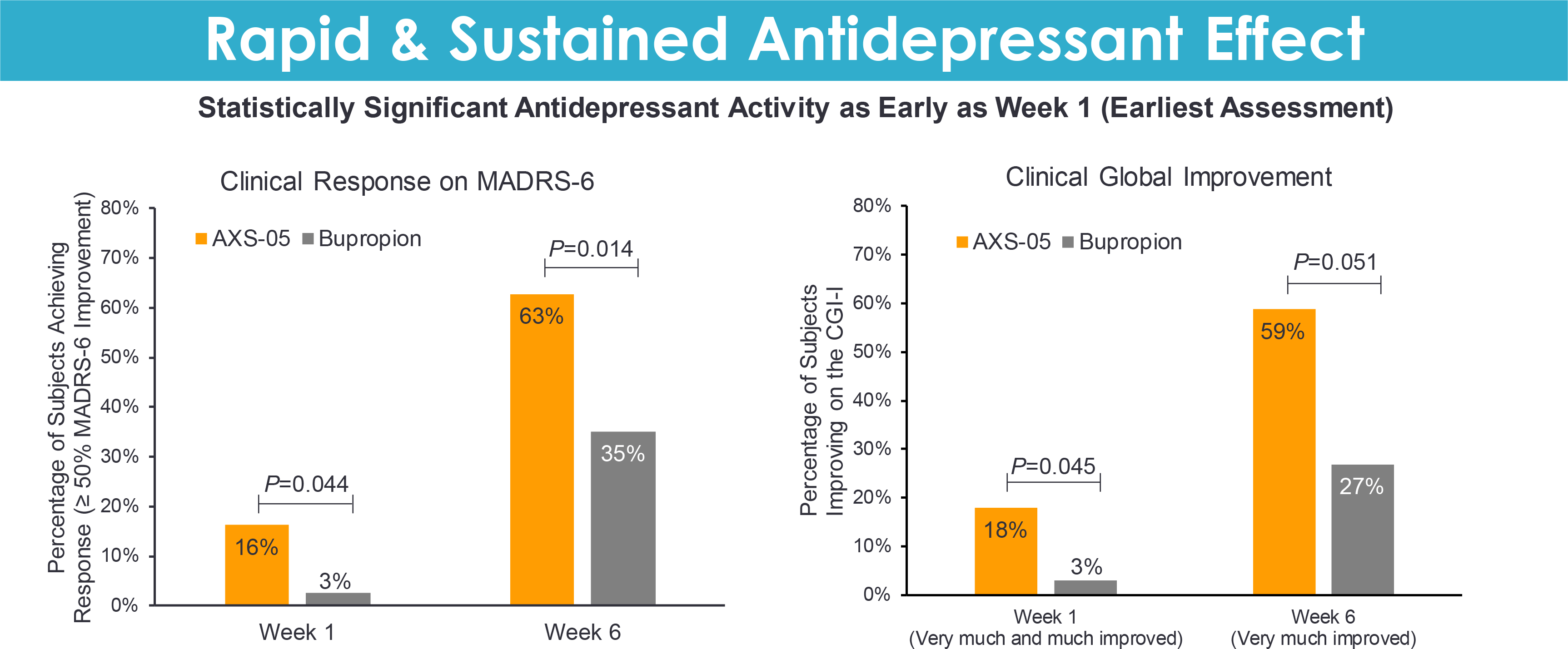
At weeks 1, 2, and 6, patients receiving dextromethorphan with bupropion showed an mean decrease in the total MADRS score of 7.4, 12.5, and 17.2 points — vs. 4.5, 7.8, and 12.1 points in the control group (p=0.169, p=0.024, p=0.013).
Clinical remission at week 6 was recorded in 47% of subjects in the dextromethorphan with bupropion group — vs. 16% in the control group (p=0.004).
Administration of Auvelity led to improvements in other measures of depression treatment effectiveness, including scores on the MADRS-6 subscale (major depression symptoms), the CGI-I scale, and the CGI-S scale.
Auvelity’s safety profile was characterized by acceptability. No adverse effects associated with psychotomimetic disturbances, weight gain, or increased sexual dysfunction were noted.
Auvelity: Market Outlook
Major depressive disorder has brought many experimental drugs to its grave. This disorder is very difficult to treat, so it is surprising how dextrometrophan with bupropion managed to easily pass the three clinical trials important for regulatory approval. Moreover, Auvelity’s therapeutic efficacy proved to be consistent in all three trials, which in the case of almost any mental disorder is virtually impossible to achieve. The problem of testing drugs for mental disorders is well known, when in one clinical trial an experimental drug works with proper efficacy, while in another, even if completely similar in design, it fails.
Thus, Auvelity, tested in the GEMINI (NCT04019704) phase 3 pivotal clinical trial, the COMET (NCT04039022) phase 2 long-term trial, and the ASCEND (NCT03595579) phase 2 additional trial, showed a 16.6, 21.1, and 17.3 point reduction in the MADRS total score after 6 weeks of treatment, or, as a percentage of baseline, by 50%, 64%, and 54%. The clinical remission of depression was achieved by 40%, 53%, and 47% of patients, respectively. And all this without much adverse events.
Long-term use of dextromethrofan with bupropion improved the proportion of patients reaching clinical remission status to 69% in 6 months of treatment. Again with no side effects.
Axsome wanted to bolster confidence in the therapeutic validity of Auvelity by proving that it was also successful in treating treatment-resistant depression (when two or more lines of therapy with different standard antidepressants fail), but it did not work out particularly smoothly. The STRIDE-1 (NCT02741791) phase 3 clinical trial comparing the drug to bupropion was unable to demonstrate a statistically significant outperformance of the experimental treatment. The problem was not with Auvelity itself but with flaws in the study design that led to insufficient statistical power. A subsequent MERIT (NCT04608396) phase 2 confirmed that Auvelity had the ability to delay the time of onset and prevent relapse of depressive symptoms. The COMET-TRD cohort in COMET (NCT04039022) also showed proper therapy efficacy. However, Axsome does not currently consider dextrometrophan with bupropion for treatment-resistant depression.
Axsome has verified that Auvelity is suitable for treating other clinically relevant patient groups: major depressive disorder not responding to one line of therapy with standard antidepressants, and major depressive disorder with suicidal ideation. The respective COMET-AU and COMET-SI cohorts in COMET (NCT04039022) confirmed this: after 6 weeks of treatment, remission was reported in 40% and 50% of patients; suicidal ideation disappeared in 60% of patients already in the first week of therapy.
In parallel, Axsome continues to evaluate Auvelity in the treatment of agitation in Alzheimer’s disease and the treatment of nicotine addiction. For example, in the ADVANCE (NCT03226522) phase 2/3 clinical trial, the baseline total score on the Cohen-Mansfield Agitation Inventory (CMAI) was reduced by nearly half, and in the NCT03471767 phase 2 clinical trial dextromethorphan with bupropion provided greater reduction in the number of cigarettes smoked and greater reduction in smoking intensity compared to administration of bupropion alone, an approved smoking cessation treatment.
Despite Auvelity’s impressive successes, there is a fly in the ointment that investors are unlikely to be happy about.
Auvelity is a combination of two generic drugs, dextromethorphan and buproprion, patented until 2040, and although the company claims that the proposed drug mix is protected by intellectual property rights, this patent position is still rather weak.
Then again, there could be problems on the part of health insurers: Would Auvelity get on formularies if Axsome charged a premium price for the drug relative to the two generic components in the composition?
On the other hand, the Auvelity business model is well-tested by other pharmaceutical manufacturers: take two existing drug compounds that were previously thoroughly and deeply scientifically studied and already implemented in clinical practice, and then, by combining them, redirect them to another therapeutic indication, quickly bringing a new drug to the market. This often works, because high innovation, accompanied by the search and development of fundamentally new molecules, requires huge budgets.
The fact that Axsome has succeeded in targeting the NMDA receptor is remarkable in itself. For instance, rapastinel and AV-101 by Allergan and VistaGen Therapeutics failed, although the latter has not given up trying to combine AV-101 with probenecid, which many times increases the concentration of this molecule in the brain.
Auvelity’s therapeutic efficacy against major depressive disorder is most likely due not just to the effects of dextromethorphan with delayed metabolism but also to synergism from bupropion.
By the way, mechanistically Auvelity is very similar to Nuedexta (dextromethorphan + quinidine), in which low-dose quinidine, acting as a CYP2D6 inhibitor, increases the plasma concentration of dextromethorphan, and which is approved in the therapy of pseudobulbar affect (PBA).
Avanir Pharmaceuticals, the company behind Nuedexta, was bought by Japan’s Otsuka Pharmaceutical in late 2014 for $3.5 billion. Avanir is continuing clinical development of the experimental AVP-786, which combines dextromethorphan modified with deuterium chemistry to improve metabolism (invented by Concert Pharmaceuticals) and low-dose quinidine. AVP-786 is being studied in the therapy of agitation associated with dementia of the Alzheimer’s type, negative symptoms of schizophrenia, neurobehavioral disinhibition in traumatic brain injury, intermittent explosive disorder.
Industry observers estimate that Auvelity won’t cross the half-billion-dollar annual sales threshold until 2026. Such restrained projections are apparently due to delays in the regulatory verdict. Obviously, once the drug is approved, financial expectations will improve dramatically. What to say, if before the regulatory problems, Auvelity’s sales forecast was exceptionally optimistic; in 2026, sales of the drug were supposed to reach $1.3 billion per year.
Auvelity is doing well in terms of intellectual property protection: The proprietary combination of dextromethorphan and buprion is securely patented until 2037–2040.
Extras
Auvelity (dextromethorphan +bupropion). Prescribing information. U.S. [PDF]
Auvelity (dextromethorphan +bupropion). FDA approval investor call. August 19, 2022. [PDF]
Axsome Therapeutics. Corporate presentation. January 2022. [PDF]
Efficacy and safety of AXS-05 (dextromethorphan-bupropion) in patients with major depressive disorder: A phase 3 randomized clinical trial (GEMINI). J Clin Psychiatry. 2022 May 30;83(4):21m14345. [source]
Effect of AXS-05 (dextromethorphan-bupropion) in major depressive disorder: A randomized double-blind controlled trial. Am J Psychiatry. 2022 May 18;appiajp21080800. [source]
Axsome Therapeutics. Novel approaches to address treatment resistant depression: Targeting multiple mechanisms of action. R&D day. April 24, 2018. [PDF]
AXS-05 for neuropsychiatric disorders: Scientific rationale and clinical development. American Society of Clinical Psychopharmacology (ASCP) 2018. [PDF]
AXS-05: A mechanistically novel oral therapeutic in development for neuropsychiatric disorders. American Psychiatric Association (APA) 2019. [PDF]
Efficacy and safety of AXS-05, an oral NMDA receptor antagonist with multimodal activity, in major depressive disorder: Results of a phase 2, double-blind, active-controlled trial. ASCP 2019. [PDF]
Efficacy and safety of AXS-05, an oral NMDA receptor antagonist with multimodal activity, in major depressive disorder: Results from the GEMINI phase 3, double-blind, placebo-controlled trial. ASCP 2020. [PDF]
Sustained efficacy and long-term safety of AXS-05, an oral NMDA receptor antagonist, in major depressive disorder: COMET study results.ASCP 2021. [PDF]
Sustained effects of AXS-05, an oral NMDA receptor antagonist, in treatment resistant depression patients: Results from the COMET-TRD trial. ASCP 2021. [PDF]
Rapid reduction in suicidal ideation in oatients treated with AXS-05, an oral NMDA receptor antagonist with multimodal activity: Results from the COMET-SI trial. ASCP 2021. [PDF]
ADVANCE-1 phase 2/3 trial of AXS-05 in Alzheimer’s disease agitation: Topline results. April 27, 2022. [PDF]