SUMMARY
- Parkinson’s disease is a common and debilitating neurodegenerative disorder.
- No drug can stop the steady progression of Parkinson’s with increasing disability.
- GLP1R agonists, which are widely used in the treatment of diabetes and obesity, have opened up from an unexpected angle.
- Drugs such as semaglutide have a neuroprotective effect that may slow the deterioration of motor function in Parkinson’s.
- GLP1R agonists are also being investigated for the treatment of non-alcoholic steatohepatitis (NASH), Alzheimer’s disease, stroke, and alcoholism.
WHAT HAPPENED
The addition of Adlyxin/Lyxumia (lixisenatide) to standard therapy for Parkinson’s disease resulted in a deceleration of the decline in motor functions, such as limb tremor, slowness and stiffness of movement, and difficulty with balance.
Lixisenatide is a glucagon-like peptide 1 receptor (GLP1R) agonist, belonging to the same class as extremely popular Ozempic (semaglutide), Wegovy (semaglutide), Mounjaro (tirzepatide), and Zepbound (tirzepatide). These drugs were developed by Novo Nordisk and Eli Lilly for the treatment of type 2 diabetes mellitus and obesity.
Adlyxin/Lixumia, once promoted by Sanofi, is no longer marketed. The French pharmaceutical giant has abandoned it due to the availability of more advanced and easier to use GLP1R agonists from other pharmaceutical manufacturers, including the ones mentioned above.
WHY IT MATTERS
Parkinson’s disease (PD) is a neurodegenerative disease that is common, debilitating, and disabling. Its best-known signs are resting tremor, limb stiffness, and slowness of movement, accompanied by complications such as vegetative symptoms, sleep disturbance, and cognitive impairment. The disease progresses steadily, resulting in increasing disability that is beyond the scope of any existing pharmacological treatments [1]. The development of neuroprotective therapies capable of slowing, halting, or reversing neurodegeneration in PD has long been a priority [2].
In his 1817 publication, “An Essay on the Shaking Palsy,” James Parkinson optimistically wrote that although the nature of the disease was unknown to him, “there appears to be sufficient reason for hoping that some remedial process may ere long be discovered, by which, at least, the progress of the disease may be stopped” [3]. However, more than two centuries have passed, and we are still waiting for this discovery.
WHAT IT FOUND OUT
The LixiPark (NCT03439943) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled French patients (n=156) aged 40–75 years with early Parkinson’s disease (Hoehn and Yahr stage < 3), who adhered to standard antiparkinsonian dopaminergic therapy and were additionally treated with daily subcutaneous injections of lixisenatide or placebo for 12 months.
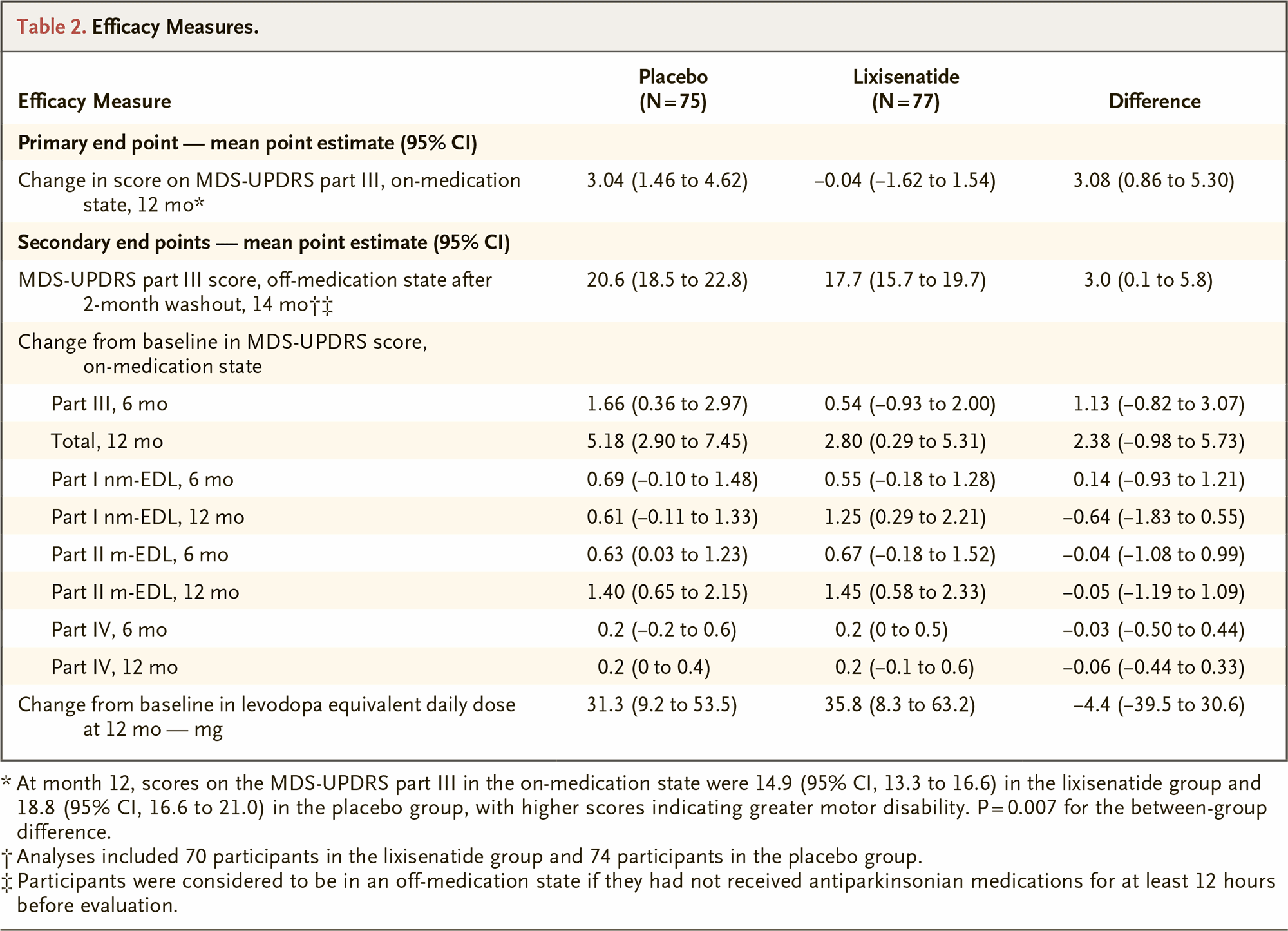
The study evaluated the efficacy of treatment by measuring the change in scores on the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part III. The lixisenatide group showed an improvement in motor function with a change of −0.04 points, while the control group showed a worsening of disability with a change of +3.04 points. The difference between the two groups was statistically significant at 3.08 points (95% CI [hereafter]: 0.86–5.30; p=0.007) [1].
After the 2-month washout period, the discrepancy persisted, even when patients were not taking any antiparkinsonian medication. The mean MDS-UPDRS motor scores were 17.7 points (15.7–19.7) — vs. 20.6 (18.5–22.8) [lower scores indicate better outcomes].
Administration of lixisenatide was followed by nausea and vomiting in 46% and 13% of subjects, respectively.
ESSENCE
The GLP1R agonist, lixisenatide, had a moderately beneficial effect on slowing the progression of motor disability in Parkinson’s disease, possibly due to its neuroprotective effects. This effect is expected to be more pronounced in patients under the age of 60 and in the early stages of the disease. However, it cannot be ruled out that there is a symptomatic effect. Studies on the GLP1R agonist exenatide in alcohol and cocaine addiction have shown that it increases synaptic dopamine levels [1] [2].
HOWEVER
Due to the limited nature of the clinical trial for the treatment of Parkinson’s disease with the GLPR1 agonist lixisenatide, it is impossible to determine whether the drug’s beneficial effect on motor function will persist with longer treatment duration or in more severe cases of the disease. Additionally, the effect size of higher or lower doses of lixisenatide remains unknown.
HOW IT WORKS
At this stage, it is speculated that GLP1R agonists may aid in the treatment of Parkinson’s disease (PD), based on relevant scientific findings. Type 2 diabetes mellitus is a risk factor for PD [1], and treatment with GLP1R agonists is associated with a reduction in this risk by over 50% [2]. In animal models of PD, GLP1R agonists have demonstrated neuroprotective effects [3]. GLP1R activation has been observed to have various physiological effects, including reducing inflammation in the brain, which is central to the pathophysiology of PD [4]. It is believed that GLP1R activation stimulates neurogenesis and protects neurons from cytokine-mediated apoptosis. This is achieved by preventing microglial conversion of astrocytes into a neurotoxic phenotype [3] [5].
WHAT’S NEXT
Most Parkinson’s patients are not concerned about their current condition, but rather about the fear of progression of motor impairment. If the maximum improvement in motor function achievable with GLP1R agonists is only 3 points on the MDS-UPDRS part III scale, then the value of such treatment is negligible, especially given the onerous gastrointestinal adverse events. However, if the therapy’s benefits demonstrate a cumulative nature, such as an annual increase of 3 points for 5–10 years or more, we can confidently assert that the world’s first treatment for transforming and altering the course of Parkinson’s disease has emerged. Long-term clinical trials are necessary [1].
BEFORE TOO LONG
In the second half of 2024, the results of Exenatide PD3 (NCT04232969) will provide more clarity on the GLP1R agonist treatment of Parkinson’s disease (PD). This phase 3 clinical trial administered exenatide, a GLP1R agonist commercialized by AstraZeneca as the antidiabetic Bydureon, by weekly subcutaneous injection for 2 years to patients (n=194) aged 25–80 years with early PD (Hoehn and Yahr stage ≤ 2.5) adhering to standard antiparkinsonian therapy.
IN EARLIER TIMES
Previous clinical trials of exenatide and experimental NLY01, a pegylated version of exenatide by Neuraly, have yielded mixed results for the treatment of Parkinson’s disease, depending on patient characteristics [1] [2] [3].
ONE MORE THING
South Korea’s Peptron hatched grand plans for experimental PT320, a sustained-release formulation of exenatide made with its proprietary SmartDepot technology based on biodegradable polymer microsphere carriers that allows the drug to be administered by subcutaneous injection once every two weeks [1] [2] [3] [4]. However, the phase 2 clinical trial NCT04269642 among patients with early Parkinson’s disease, which began in spring 2020, has not yet been completed.
MEANWHILE
GLP1R agonists have been shown to provide benefits beyond the treatment of type 2 diabetes mellitus and obesity alone.
Thus, semaglutide, promoted by Novo Nordisk, has been shown to, first, reduce the risk of adverse cardiovascular outcomes in obesity-associated cardiovascular disease and, second, to be successful in the treatment of heart failure with preserved ejection fraction (HFpEF) among obese patients [1] [2]. This was predictable, however, given how overweight is toxic to the cardiovascular system.
Semaglutide was also able to restrain the progression of chronic kidney disease (CKD) and reduce the risk of cardiovascular and renal death in patients with type 2 diabetes [3].
In summer 2024, Eli Lilly will reveal to what extent Zepbound (tirzepatide) is therapeutically relevant in HFpEF with comorbid obesity. This question is being uncovered in the SUMMIT (NCT04847557) phase 3 clinical trial.
By the fall of 2025, it will be determined whether semaglutide is suitable for the treatment of Alzheimer’s disease (AD). Whether Rybelsus, taken daily orally for 2 years in the EVOKE (NCT04777396) phase 3 clinical trial, can slow the progression of dementia in patients with early AD.
In spring 2026, results are expected from the GALLOP (NCT05920889) phase 2 clinical trial verifying the hypothesis that adding semaglutide to the standard endovascular thrombectomy (EVT) for acute ischemic stroke caused by large vessel occlusion (LVO) prevents adverse outcomes due to peri-procedural malignant brain edema (MBE) and symptomatic intracranial hemorrhage (sICH).
The topic of non-alcoholic steatohepatitis (NASH), which is of interest to literally every Big Pharma player due to its huge business prospects, but in fact remains without really strong drugs, is being investigated in the ESSENCE (NCT04822181) phase 3 clinical trial, which is studying long-term (maximum 5 years) weekly use of injectable semaglutide in NASH without cirrhosis and with liver fibrosis at the F2–F3 stage.
Semaglutide continues to be studied in people with comorbid obesity and alcohol dependence. Whether Wegovy, which is being administered by weekly subcutaneous injection in the SEMALCO (NCT05895643) phase 2 clinical trial, can reduce alcohol consumption or even eliminate alcoholism.