Highlights
Precigen ActoBio has shared the success of a clinical trial of an experimental therapy for recently diagnosed type 1 diabetes mellitus.
At this stage, it is clear that the experimental treatment does work, and it can be done chronically; it will stabilize the disease without any serious side effects.
There are some signs of a reversal of type 1 diabetes but it is too early to declare this with certainty.
AG019 and Teplizumab for Type 1 Diabetes Mellitus: Mechanism of Action
Precigen ActoBio has developed an oral capsule, AG019, which contains Lactococcus lactis bacteria genetically engineered to deliver two components to the gastrointestinal tissue mucosa: human proinsulin (hPINS) and human interleukin 10 (hIL-10). The mechanism of action of AG019 is related to the induction of antigen-specific regulatory T cells (Tregs), which, by migrating to the inflamed tissue and blocking its destruction, reduce or eliminate the destruction of the insulin-producing beta cells of the pancreatic Langerhans islets. As a result, insulin synthesis is stabilized or improved.
- AG019 is based on ActoBiotics, a proprietary therapeutic platform, which involves genetic modification of Lactococcus lactis, a well-studied and safe food bacterium. The therapeutic gene is inserted into the L. lactis genome previously stripped of its ability to reproduce. ActoBiotics-based drugs can be made as oral capsules, buccal rinses, or topical solutions. After delivery, L. lactis starts secreting the desired proteins, peptides, or antibodies, and only locally. Production, involving fermentation, concentration, and freeze-drying, does not require costly purification processes.
Since type 1 diabetes is an autoimmune disease, in which the immune system destroys beta cells, it makes sense from a long-term therapeutic perspective to provide antigen-specific immune tolerance to islet antigens and reverse the autoimmune phenotype. In this case, hPINS acts as an antigen, and the cytokine hIL-10 is needed to increase tolerance. Due to the fact that in diabetes mellitus 1 beta cells are inevitably destroyed, the administration of AG019 (both prophylactic and therapeutic) should be done when the disease has not gone too far, that is, there is still a residual functional beta-cell mass.

Precigen ActoBio performed clinical validation not only of AG019 itself but also of its combination with experimental teplizumab (PRV-031), a humanized monoclonal antibody against CD3.
- CD3 protein is a co-receptor involved in T cell activation during the immune response. Teplizumab binds to the CD3 epsilon-chain epitope (CD3E) expressed on mature T lymphocytes thereby modulating pathological immune responses. As a result, autoreactive T cells are inhibited without affecting regulatory T cells. In other words, it organizes the possibility of restoring the state of immune tolerance, which involves restraining the attacks of T lymphocytes on beta cells.
Teplizumab, invented by MacroGenics, is being developed by Provention Bio, which hopes the U.S. Food and Drug Administration (FDA) will approve it this year, 2021, although delays of up to a year have not been ruled out. By early July, the regulator will decide. If it is positive, teplizumab will become the world’s first drug to delay or prevent the development of type 1 diabetes in people predisposed to it. Possible brand names for teplizumab are Tzield, Tprezev, or Teploneer.
Clinical Efficacy and Safety of Experimental Therapy for Type 1 Diabetes Mellitus
The NCT03751007 phase 1b/2a clinical trial invited patients aged 12–42 years with type 1 diabetes mellitus diagnosed no later than 150 days before the start of the experimental treatment. Among the main criteria for participation: the presence of autoantibodies to at least one beta-cell autoantigen (insulin, IA-2, GAD65, ZnT8) and C-peptide levels >0.2 nmol/L (by a 4-hour mixed-meal tolerance test [MMTT], reflects endogenous insulin secretion).
Phase 1b (open-label) participants (n=27) received AG019 monotherapy (daily dose for 8 weeks); phase 2a (double-blind, placebo-controlled) participants (n=18) received combination therapy of AG019 (same regimen) and teplizumab, which was administered by daily intravenous infusions for 12 days.
The safety profile of AG019 was confirmed: no serious or severe adverse reactions were detected and AG019 itself was delivered strictly locally and was characterized by neither systemic exposure of its components nor persistent bacterial colonization of the gut.
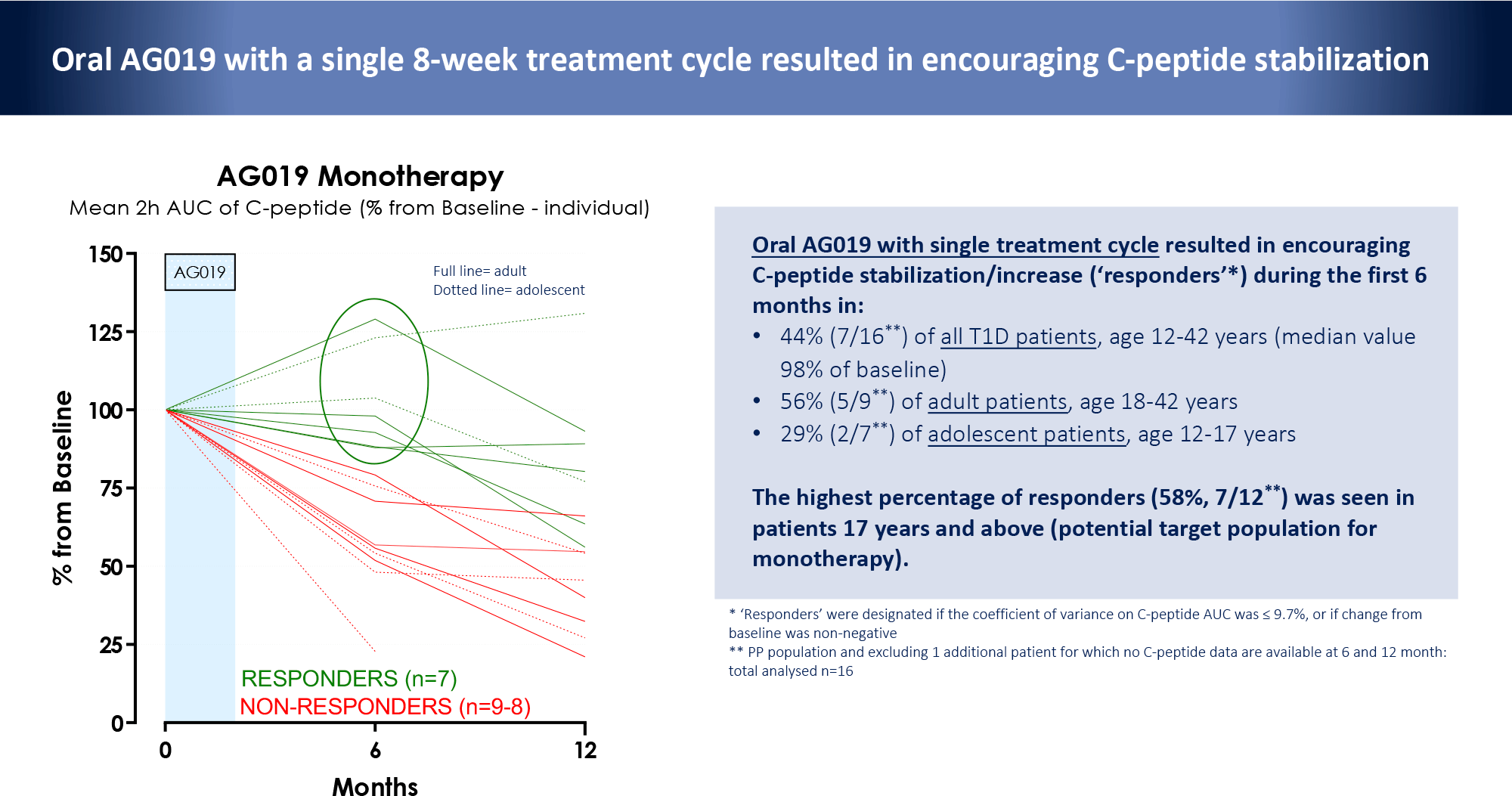
AG019 monotherapy resulted in favorable changes in C-peptide levels. In 44% (n=7/16) of all subjects (ages 12–42), 56% (n=5/9) [18–42], and 29% (n=2/7) [12–17] it stabilized or increased during the 6-month follow-up period after 8 weeks of therapy.
- Such subjects achieved respondent status: the coefficient of variance on C-peptide’s area under the curve AUC ≤ 9.7% or its non-negative change from baseline.
At the same time, the highest proportion of responders was noted among patients 17 years of age or older (58%, n=7/12) suggesting a potential target population for AG019 monotherapy.
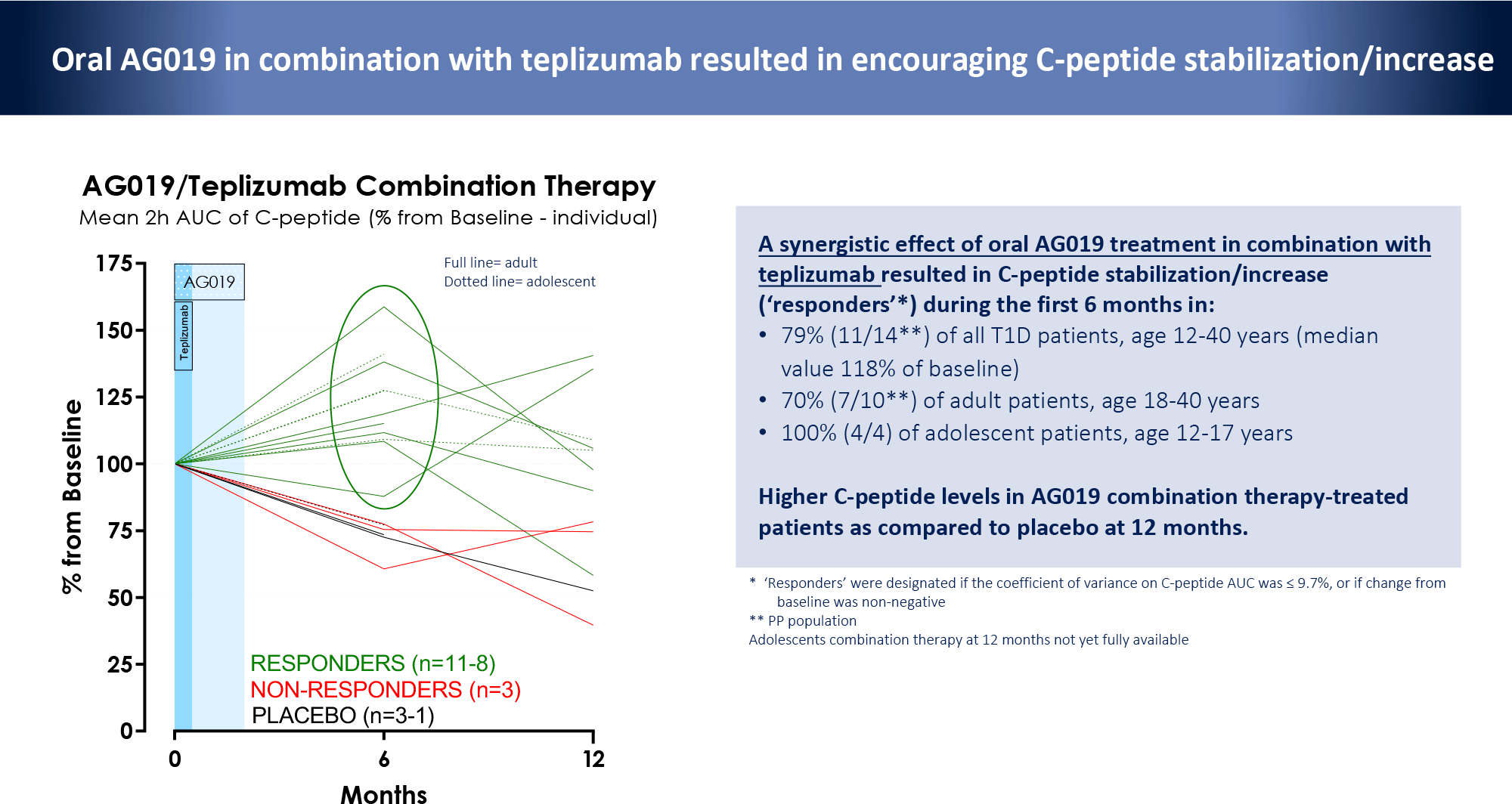
The addition of teplizumab to AG019 provided improved outcomes within the first 6 months. The responder status was 79% (n=11/14) of all subjects (ages 12–40), 70% (n=7/10) [18–40], and 100% (n=4/4) [12–17].
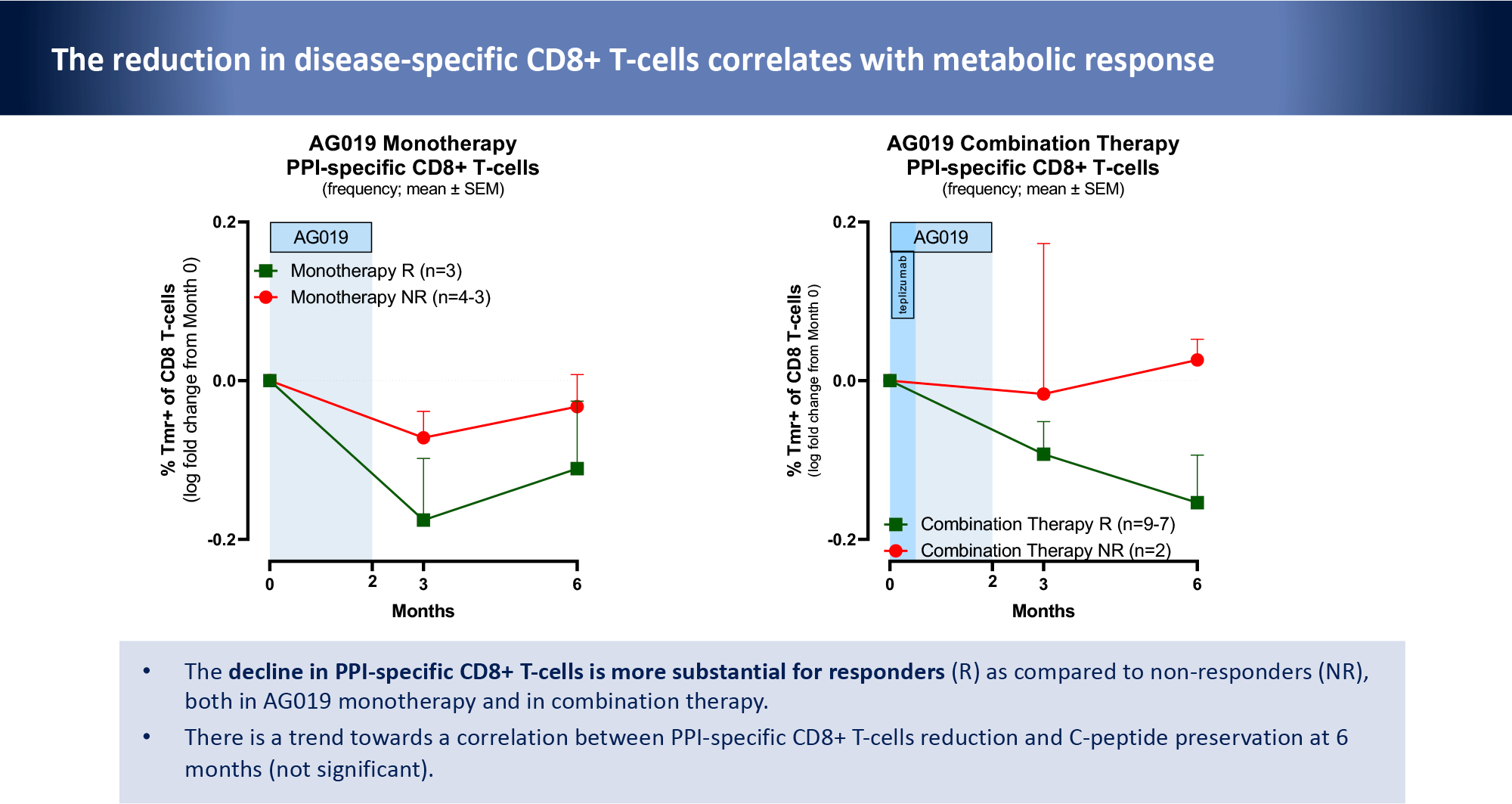
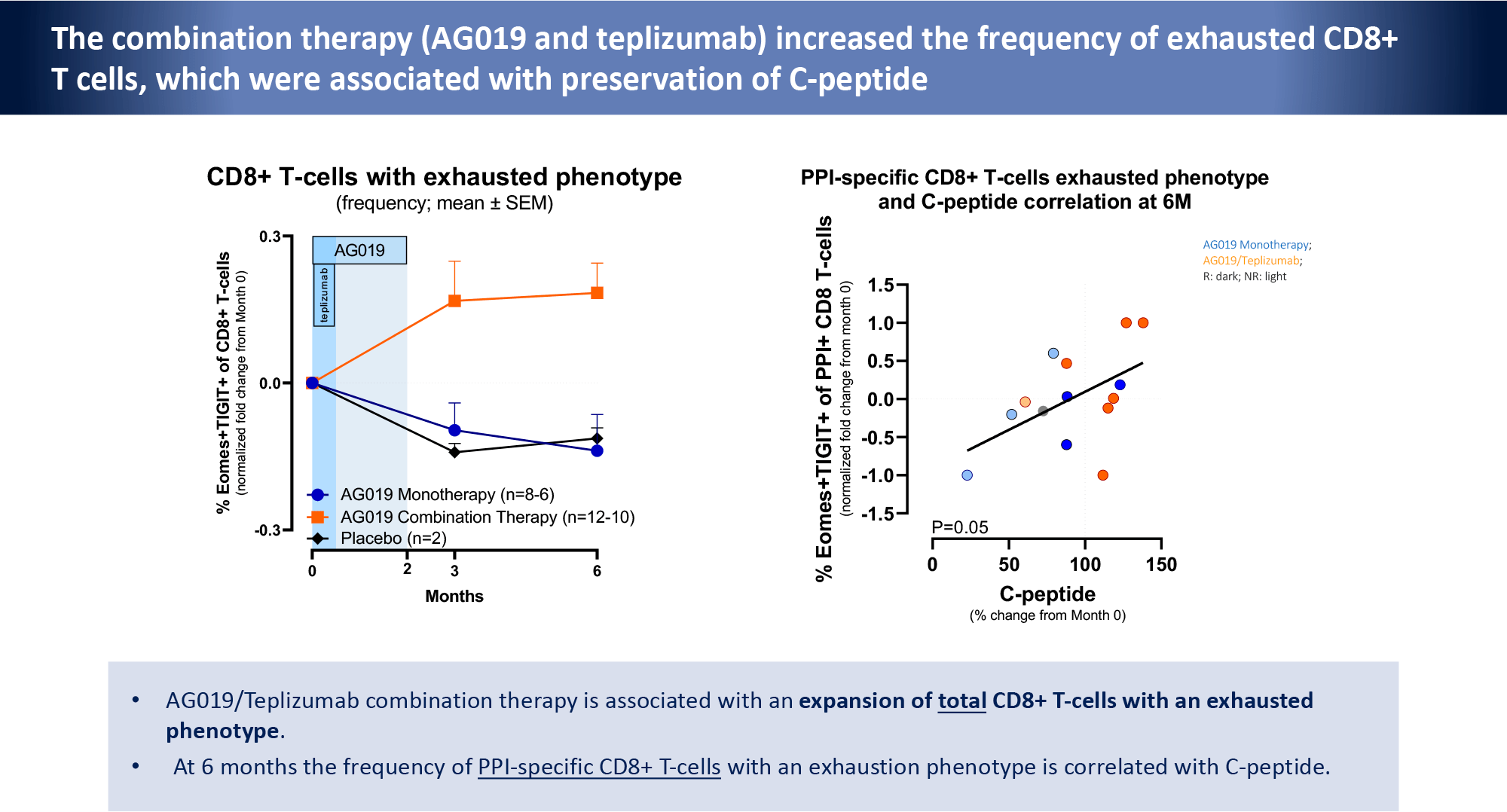
The experimental treatment was reflected by a decrease in preproinsulin (PPI)-specific CD8+ T cells concentrations. Firstly, it was stronger among responders. Secondly, there was a trend towards a correlation with preserved C-peptide levels. At the same time, combination therapy increased the frequency of PPI-specific CD8+ T cells with an exhausted phenotype.
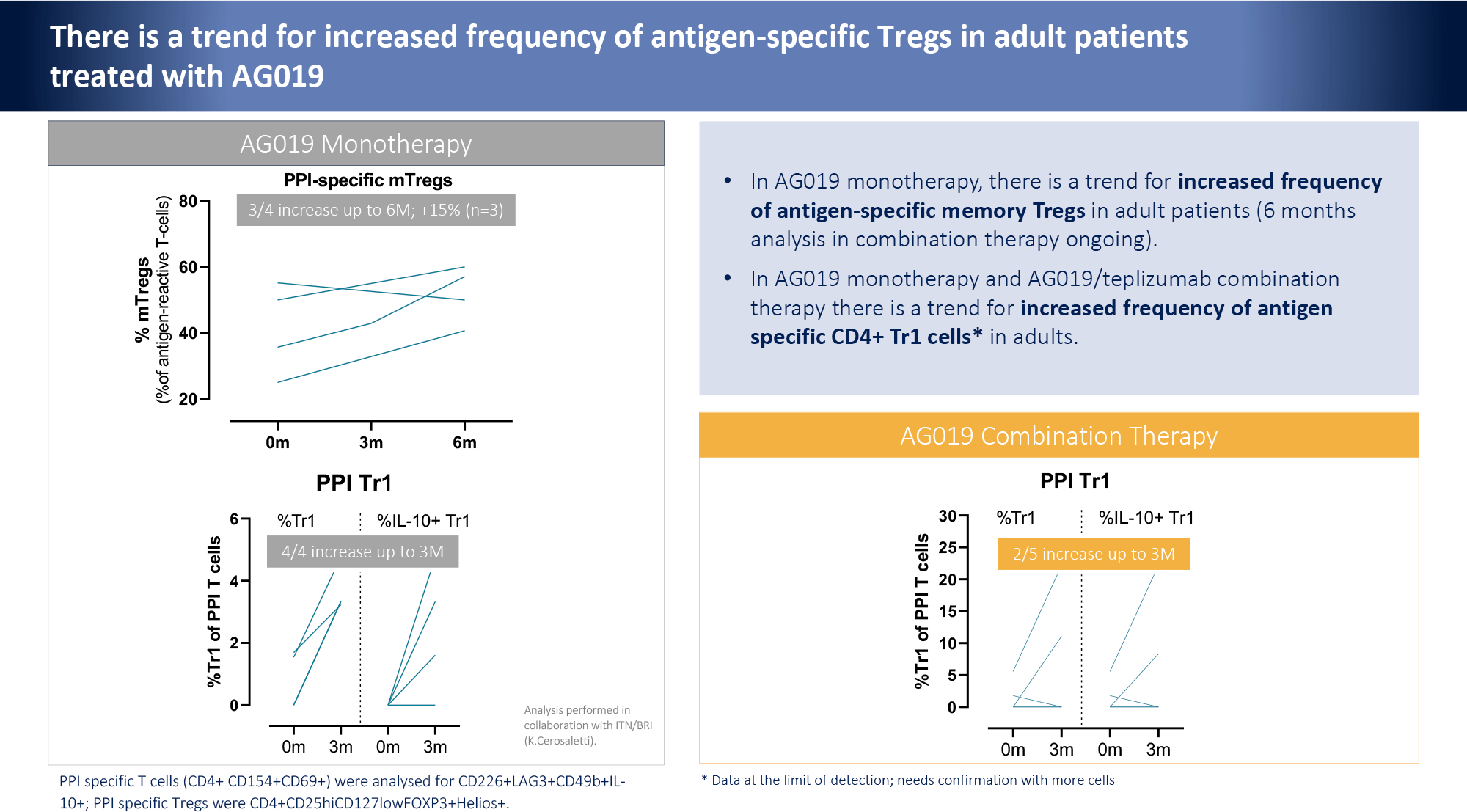
Adult patients showed trends toward increased frequencies of both PPI-reactive memory Tregs and PPI-reactive CD4+ type 1 regulatory cells (TR1).
Extras
Lactococcus lactis producing proinsulin and IL-10 increases antigen specific regulatory T-cells in monotherapy and in combination with an anti-CD3 monoclonal antibody (teplizumab) in newly diagnosed T1D patients. Precigen ActoBio. FOCIS 2021. [PDF]