SUMMARY
- Low-grade glioma (LGG) is the most prevalent central nervous system tumor in children.
- Surgical resection is a reliable method for achieving complete remission of LGG.
- However, surgical intervention is not an appropriate treatment option for all patients with LGG, necessitating the use of a prolonged course of chronic therapy that is burdensome, exhausting, and toxic.
- Ojemda (tovorafenib) is a novel drug that is anticipated to become the standard of care for first-line pharmacologic treatment of LGG.
- The administration of tovorafenib results in a rapid reduction in tumor size and is well tolerated.
WHAT HAPPENED
Ojemda (tovorafenib) is a new drug indicated for the treatment of relapsed or refractory low-grade glioma (LGG) in patients 6 months of age and older.
Ojemda is indicated exclusively in the case of LGG harboring a BRAF fusion or rearrangement, or BRAF V600 mutation.
In late April 2024, the U.S. Food and Drug Administration (FDA) approved Ojemda on a accelerated basis. This means that the efficacy of the drug has yet to be confirmed.
Ojemda is available in tablet and suspension forms and is prescribed once a week.
Tovorafenib, an oral pan-RAF kinase inhibitor, is developed by Day One Biopharmaceuticals.

WHY IT MATTERS
Low-grade glioma (LGG) is the most prevalent central nervous system tumor in children, accounting for approximately 30% of all such tumors. LGG is regarded as indolent (sluggish), with an excellent prognosis (10-year survival rate exceeding 90%) and potentially curable through complete surgical resection [1].
However, 70% of patients with LGG require systemic therapy because either the tumor is located in a critical region of the brain and therefore not amenable to surgical intervention or due to disease progression [1] [2] [3] [4] [5].
The chronic therapy for LGG, represented by chemotherapy and radiation, imposes a significant burden on the patient. Thus, weekly visits to a healthcare facility are required, and catheter placement is often necessary. It is estimated that three-quarters of patients experience severe hematologic toxicity, while one in five patients experience peripheral neuropathy. Furthermore, the risks of secondary malignancies and malignant transformation are high. Chronic treatment of LGG is associated with a number of serious adverse events, including cognitive decline, endocrine failure, vascular damage, and growth abnormalities [6] [7] [8] [9] [10] [11] [12].
To date, no pharmacological or standard therapeutic approaches have been proposed for relapsed or progressive LGG that would ensure regression and stabilization of the disease, avoid acute and long-term toxic effects (especially those limiting cognitive function) to the greatest extent possible, and provide patients with the opportunity for problem-free daily activities [13].
HOW IT WORKS
The serine-threonine RAF kinases (ARAF, BRAF, and CRAF) are components of the mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) signaling pathways. These pathways regulate a variety of cellular processes, including cell proliferation, differentiation, migration, survival, and angiogenesis [1] [2].
Low-grade glioma (LGG) is characterized by BRAF gene alterations in 70% of cases, with BRAF fusions being detected in 85% of cases and BRAF V600E mutations in 15% [3] [4] [5] [6].
Therefore, it is reasonable to propose that impaired oncogenic signaling should be blocked to treat LGG.
A number of inhibitors of the RAS/MAPK pathway, including vemurafenib and dabrafenib (BRAF inhibitors), trametinib and selumetinib (MEK1/MEK2 inhibitors), have shown efficacy in the treatment of LGG [7].
In patients with BRAF fusion disease, MEK1/MEK2 inhibitors are preferred over BRAF inhibitors due to the risk of paradoxical activation of the MAPK pathway. However, in the setting of increased RTK expression, there is a high likelihood of developing treatment resistance, highlighting the need for new drug molecules [8] [9] [10].
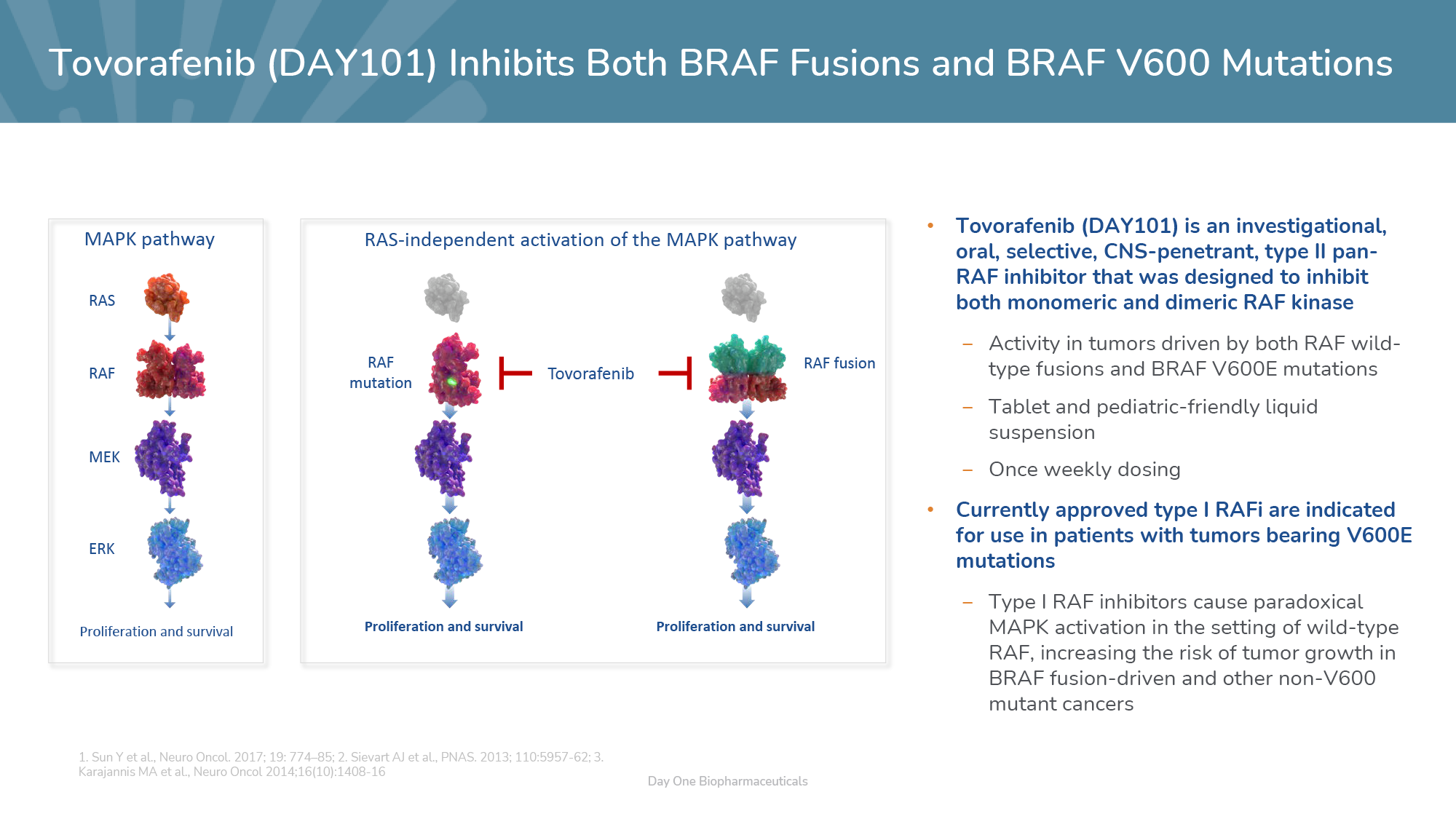
Tovorafenib (DAY101, TAK-580, MLN2480, BIIB024) is an oral small-molecule selective pan-RAF inhibitor capable of penetrating the central nervous system [11] [12] [13] [14].
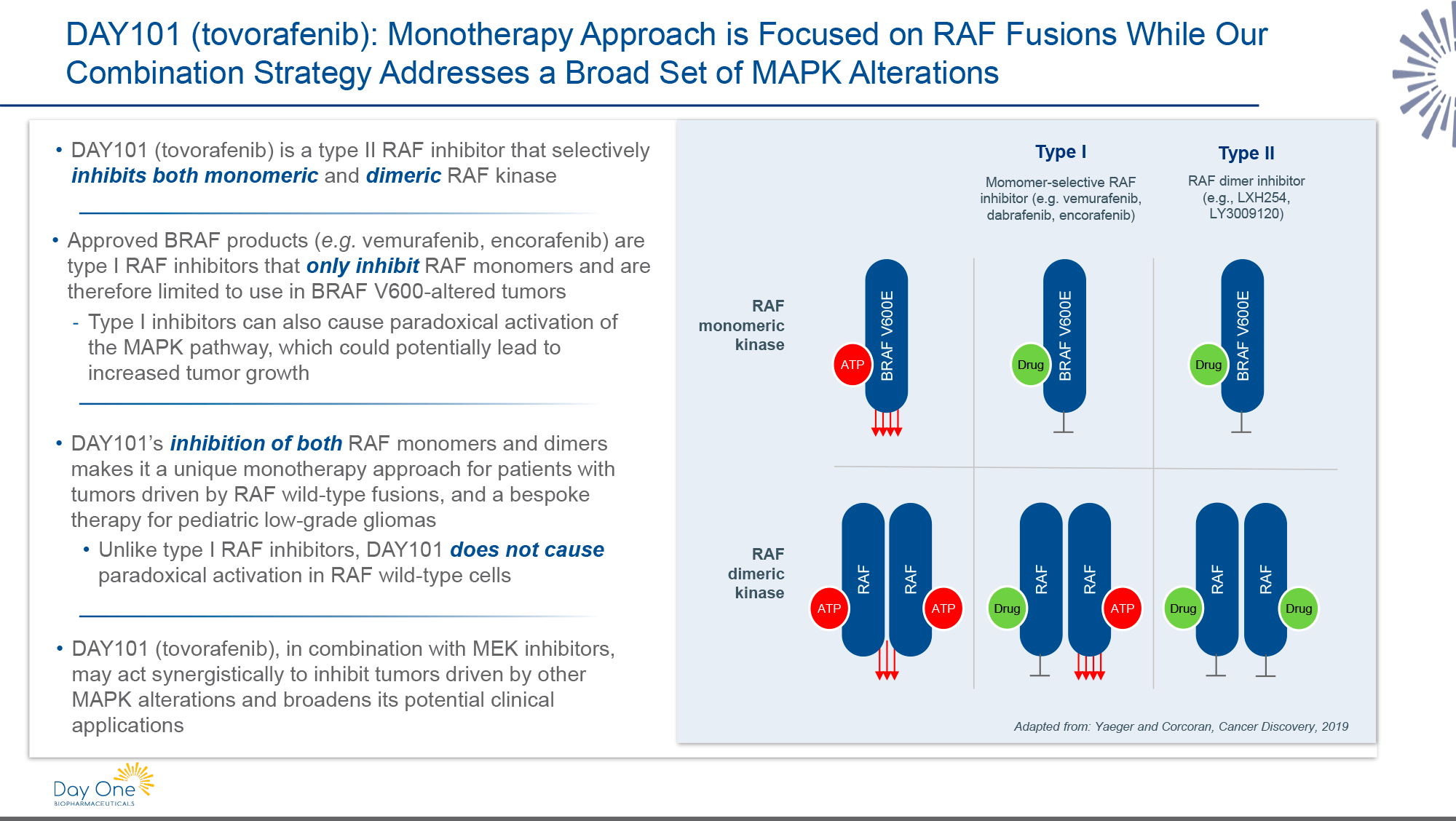
Tovorafenib belongs to the type II RAF inhibitors. Unlike existing type I BRAF inhibitors, it does not induce RAS-dependent paradoxical activation of the MAPK signaling pathway in wild-type RAF, which increases the risk of tumor growth in BRAF-associated tumors.
Tovorafenib inhibits both oncogenic RAF fusions, which signal as RAS-independent dimers, and V600E mutant BRAF, which signals as a RAS-independent monomer.
WHAT IT FOUND OUT
The pivotal FIREFLY-1 (NCT04775485) phase 2 (non-randomized, open-label, multicenter, international) clinical trial enrolled patients (n=76) aged 6 months to 25 years with recurrent or progressive low-grade glioma (LGG) with a BRAF-activating alteration. Participants must have received at least one line of systemic therapy.
Subjects were administered Ojemda (tovorafenib) orally on a weekly basis until disease progression or the development of unacceptable toxicity.
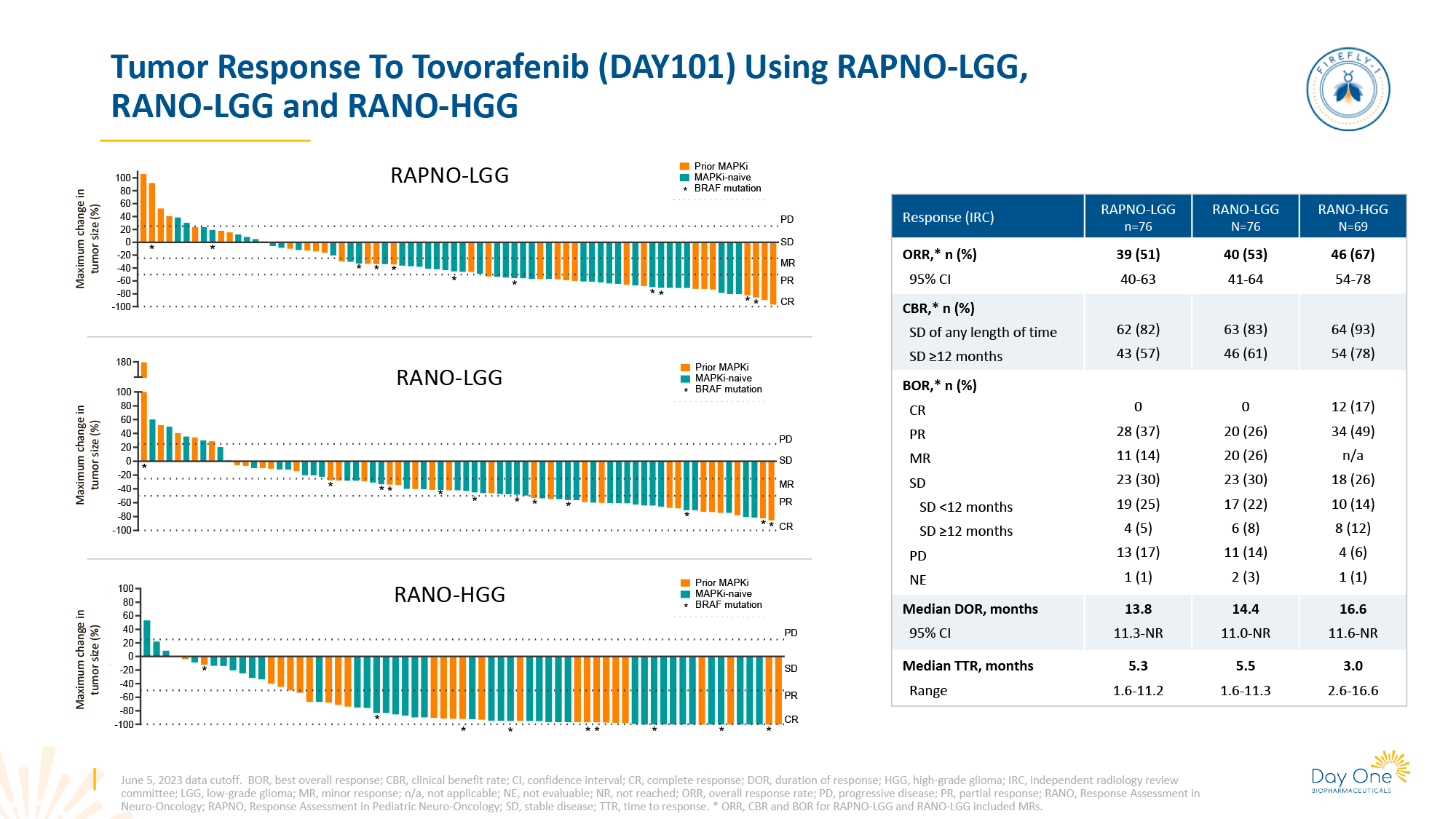
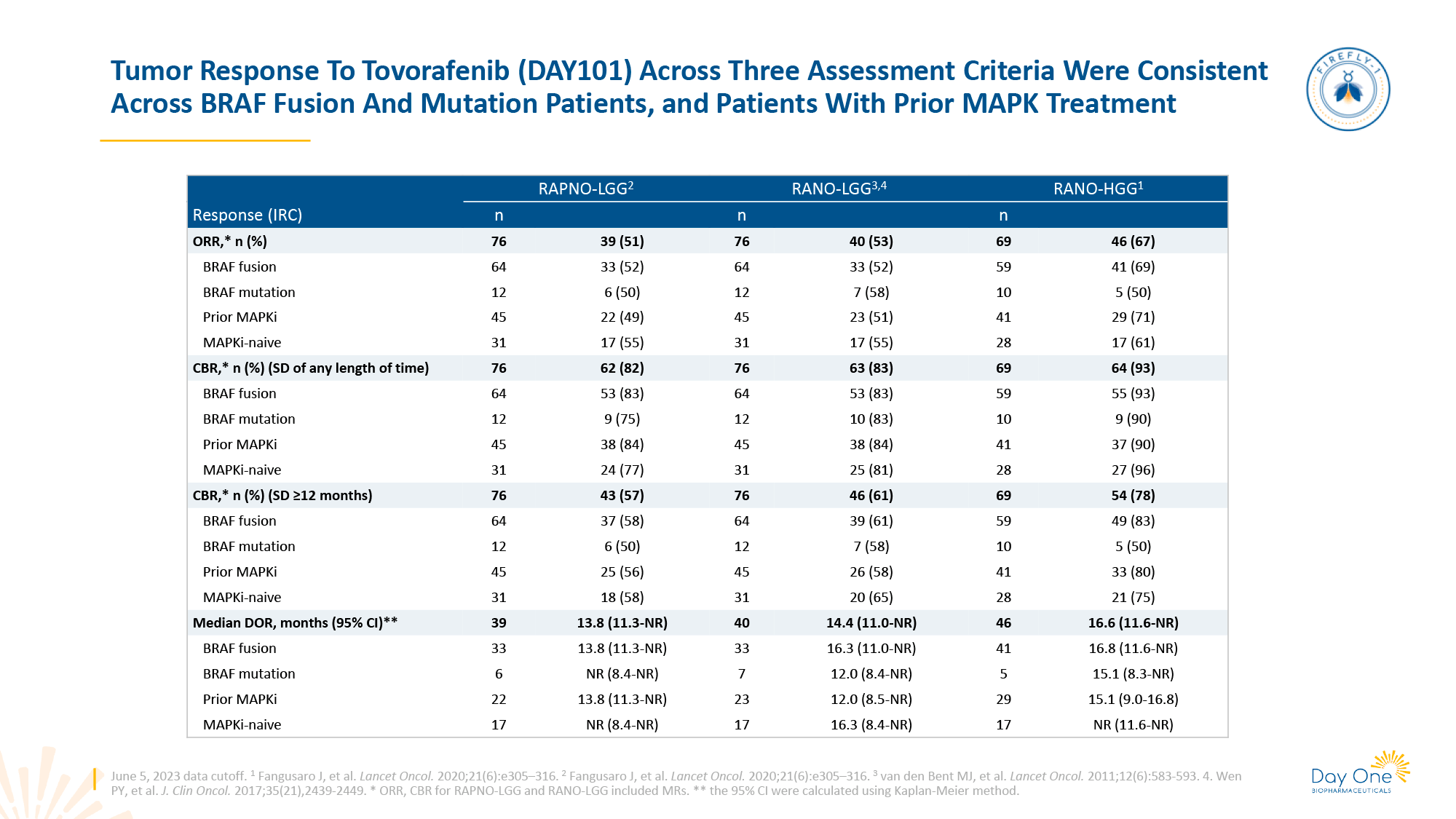
The treatment outcomes were as follows (with three values for each outcome measure according to the response assessment criteria used — RAPNO-LGG, RANO-LGG, and RANO-HGG) [1]:
- overall response rate (ORR): 51%, 53%, 67%
- complete response (CR): 0%, 0%, 17%
- partial response (PR): 37%, 26%, 49%
- minor response (MR): 14%, 26%, n/a
- clinical benefit rate (CBR): 82%, 83%, 93%
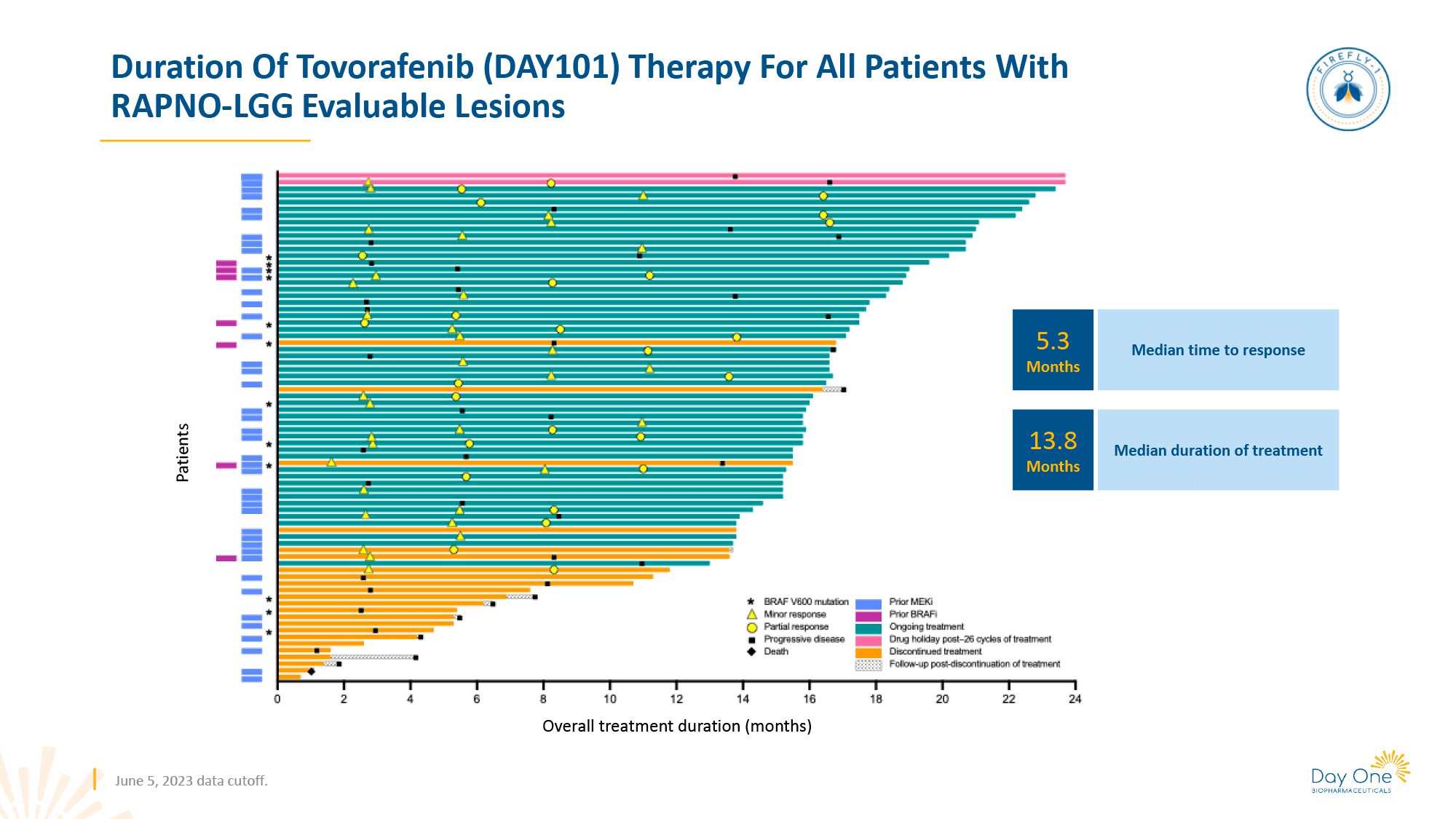
- median duration of response (DOR), months: 13.8, 14.4, 16.6
- median time to response (TTR), months: 5.3, 5.5, 3.0.
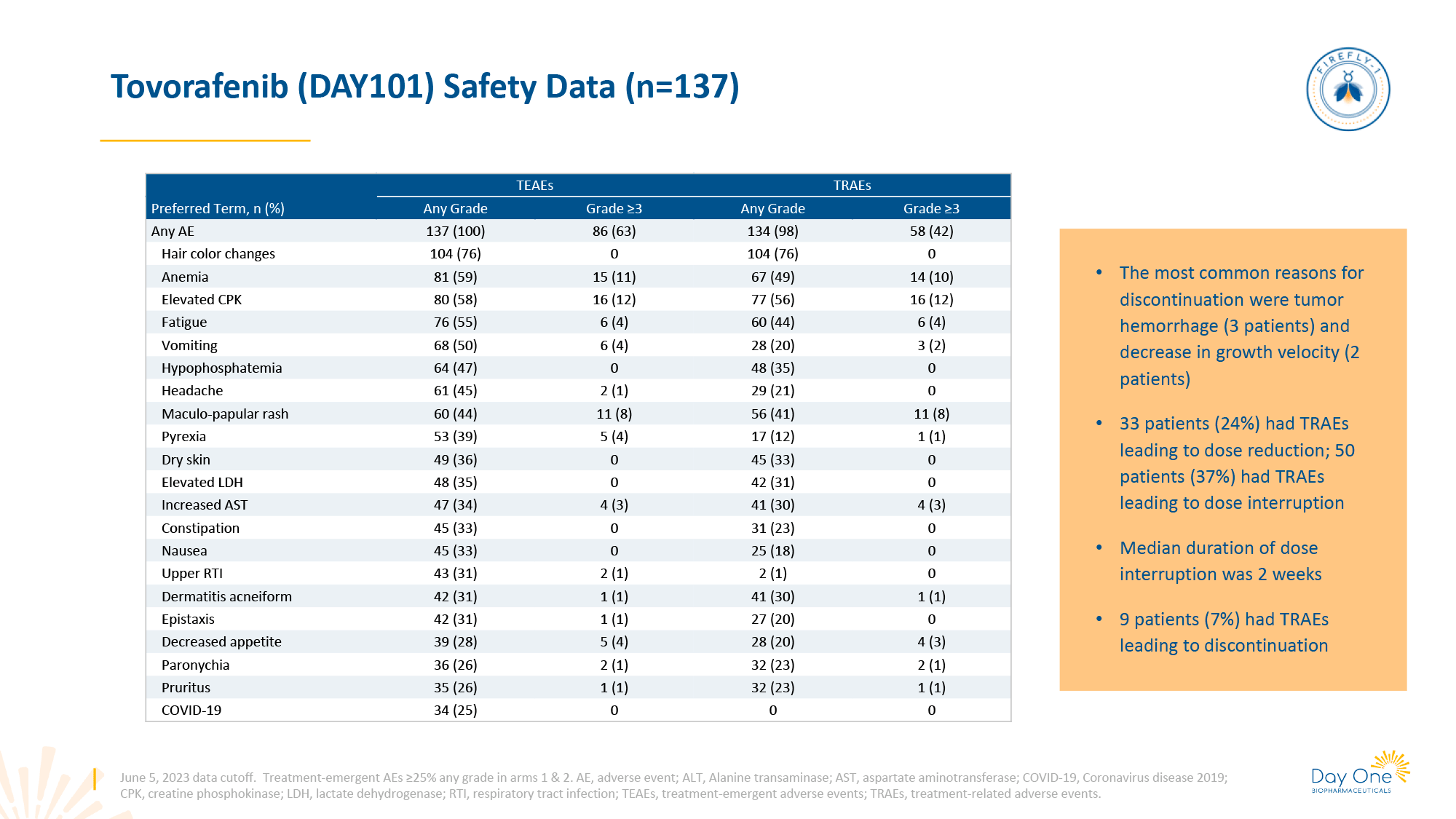
The most prevalent adverse events (AEs) were primarily of a mild to moderate severity, including rash, hair color changes, dry skin, dermatitis acneiform, pruritus, fatigue, pyrexia, edema, infections, gastrointestinal disorders, headache, hemorrhage, and laboratory abnormalities.
Due to AEs, 7% of patients had to discontinue treatment entirely, 57% had to temporarily cease treatment, and 24% had to reduce the dosage of the drug.
ESSENCE
The administration of Ojemda (tovorafenib) in the setting of recurrent or refractory BRAF-altered low-grade glioma (LGG) in pediatric and young adult patients resulted in a clinically meaningful, rapid, and durable antitumor effect.
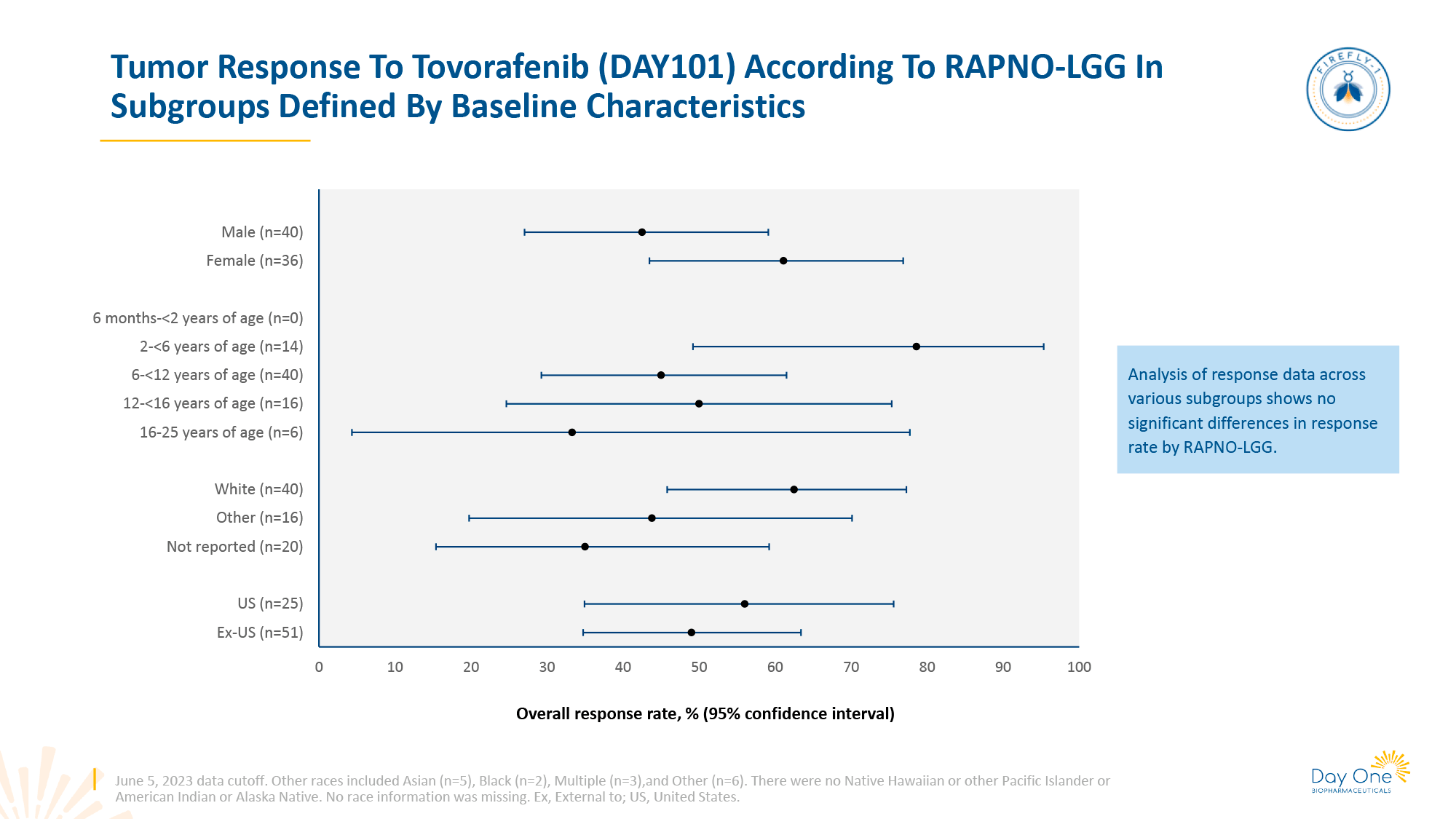
It is noteworthy that Ojemda demonstrated robust clinical efficacy, irrespective of the fact that patients had undergone an average of three lines of systemic therapy. Furthermore, over half of the patients were already receiving RAF and/or MEK inhibitors.
The therapeutic efficacy of Ojemda was evaluated using three distinct radiologic response assessment criteria: Response Assessment in Pediatric Neuro-Oncology Low-Grade Glioma (RAPNO-LGG), Response Assessment in Neuro-Oncology Low-Grade Glioma (RAPNO-LGG), and Response Assessment in Neuro-Oncology High-Grade Glioma (RANO-HGG).
The RAPNO-LGG and RANO-LGG criteria assess tumor response to treatment by the absence of disease worsening primarily on T2-weighted fluid-attenuated inversion recovery (FLAIR) images, whereas the RANO-HGG criteria assess response on T1-weighted gadolinium-enhanced images.
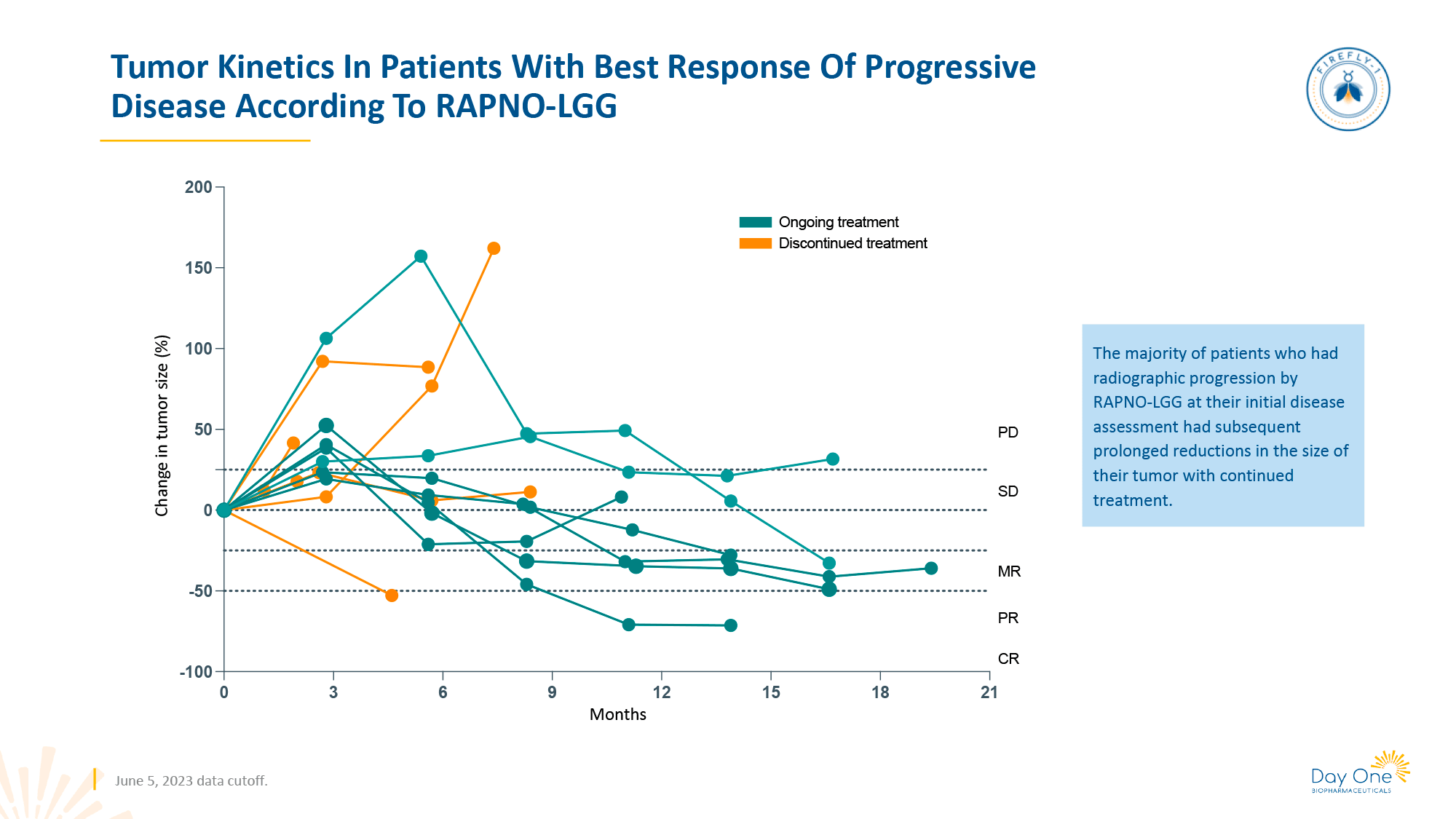
The primary endpoint of treatment efficacy in the FIREFLY-1 study (NCT04775485) was established by the overall response rate (ORR) according to the RANO-HGG criteria. However, reduction in the size of contrast-enhanced tumor may not always reflect all aspects of antitumor activity of therapy, especially since pediatric LGG is characterized by somewhat different clinical and biological features than adult LGG. For this reason, the RAPNO-LGG and RANO-LGG criteria were included as secondary endpoints for ORR, taking into account additional details such as changes in tumor-associated cysts, minor response (25%–49% tumor shrinkage), and changes in the tumor-affected optic tract and hypothalamus.
Although the response to Ojemda was typically rapid, in some patients it was delayed. Following an initial increase in tumor size (due to transient infiltration by immune cells), there was a subsequent marked reduction in tumor size. In other words, in the event of early radiological progression of the disease but without corresponding clinical signs, a repeat MRI scan after 8–12 weeks is recommended.
The safety and tolerability profile of Ojemda was found to be highly acceptable, with only a few instances of severe adverse events (AEs) observed. No evidence of ophthalmologic toxicity, adverse cardiac effects, or abnormal weight gain — AEs commonly associated with MEK inhibitors — was identified.
KEY TAKE-AWAYS
Ojemda (tovorafenib) has demonstrated clear superiority over traditional MEK and BRAF inhibitors in terms of clinical efficacy, CNS penetration, low risk of treatment resistance, infrequent weekly dosing, and manageable adverse events.
However, to definitively confirm the therapeutic validity of Ojemda for low-grade glioma (LGG), long-term follow-up is required, along with direct clinical comparisons with existing drugs. It is also important to consider the issue of toxicity associated with long-term therapy.
WHAT’S NEXT
Day One Biopharmaceuticals is continuing its efforts to expand the range of patients eligible for Ojemda (tovorafenib).
Thus, the FIREFLY-2 (NCT05566795) phase 3 clinical trial comparing the administration of tovorafenib with standard chemotherapy (either vincristine + carboplatin or vinblastine) in the first-line treatment of the same patient population as in FIREFLY-1 (NCT04775485), i.e. with RAF-altered low-grade glioma (LGG), is ongoing.
Enrollment of participants with recurrent, progressive or refractory solid tumors with aberrations of the MAPK pathway (RAS, RAF, MEK, or NF1 genomic alterations) in the FIRELIGHT-1 (NCT04985604) phase 1b/2 clinical trial continues. It is evaluating the combination of tovorafenib and pimasertib, an oral small-molecule selective MEK1/2 inhibitor licensed from Merck KGaA in February 2021, which is characterized by almost three times greater ability to penetrate the CNS than other MEK inhibitors such as trametinib or selumetinib [1] [2] [3] [4].
CHALLENGING ENDEAVOUR
The fate of tovorafenib is not straightforward. Over the years of its existence, the molecule has been transferred from one developer to another, changing its code names along the way.
Thus, tovorafenib (BIIB024) was initially developed by Biogen and Sunesis Pharmaceuticals, which joined forces in September 2004 [1] [2]. The latter merged with Viracta Pharmaceuticals in February 2021 [3].
Following the decision by Biogen to redirect its focus towards neuroscience in November 2010, which effectively resulted in the abandonment of its other business interests [4], tovorafenib (MLN2480) underwent a change in ownership in April 2011, transferring to Millennium Pharmaceuticals [2]. This company had been owned by Takeda Pharmaceutical since May 2008, having been acquired for a sum of $8.8 billion [5]. The Japanese pharmaceutical giant has, in fact, put the investigational drug (TAK-580) aside, although it has attempted to consolidate it, including in the treatment of melanoma [6].
Day One Biopharmaceuticals, which emerged in May 2020 with $60 million in venture capital funding, boldly declared a promising future for tovorafenib (DAY-101) [7], which it licensed from Takeda in September 2019 [8]. By the end of May 2021, the company had become a publicly traded entity and conducted an initial public offering (IPO) of $184 million [8]. In June 2022, the positive data of a phase 2 clinical trial of tovorafenib were released, resulting in a 125% increase in stock prices [9]. In June 2023, when even more encouraging data were presented, investors fully believed in the success of tovorafenib [10].
EXTRAS
Corporate
Corporate Presentation. Day One Biopharmaceuticals. February 2024. [PDF]
Day One Biopharmaceuticals. JPM 2024. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. October 2023. [PDF]
ASCO 2023 Conference Call. Day One Biopharmaceuticals. June 2023. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. March 2023. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. November 2022. [PDF]
Initial Data from Pivotal FIREFLY-1 Trial of Tovorafenib (DAY101) in Relapsed Pediatric Low-Grade Glioma. Investor Call. Day One Biopharmaceuticals. June 2022. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. June 2022. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. May 2022. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. April 2022. [PDF]
Corporate Presentation. Day One Biopharmaceuticals. January 2022. [PDF]
Medical Conferences
Preclinical activity of the type II RAF inhibitor tovorafenib in tumor models harboring either a BRAF fusion or an NF1-LOF mutation. AACR 2024. [PDF]
Clinical activity and safety of tovorafenib in patients with optic pathway gliomas in FIREFLY-1. ASPHO 2024. [PDF]
Clinical activity of RAF inhibitor tovorafenib according to prior MAPK inhibitor treatment in the registrational low-grade glioma arm of the phase 2 FIREFLY-1 (PNOC026) study. SNO 2023. [PDF]
Clinical activity and safety of the RAF inhibitor tovorafenib in patients with optic pathway gliomas in the registrational pediatric low-grade glioma arm of the phase 2 FIREFLY-1 (PNOC026) study. SNO 2023. [PDF]
Preliminary clinical activity of the type II RAF inhibitor tovorafenib in RAF fusion-driven recurrent/progressive sarcomas. CTOS 2023. [PDF]
Clinical activity of pan-RAF inhibitor tovorafenib in the registrational pediatric low-grade glioma arm of the phase 2 FIREFLY-1 (PNOC026) study. SNO 2023. [PDF]
Clinical activity of pan-RAF inhibitor tovorafenib in the registrational pediatric low-grade glioma arm of the phase 2 FIREFLY-1 (PNOC026) study. ASCO 2023. [PDF]
LOGGIC/FIREFLY-2: A phase 3, randomized trial of tovorafenib vs. chemotherapy in pediatric and young adult patients with newly diagnosed low-grade glioma harboring an activating RAF alteration. ASCO 2023. [PDF]
Healthcare resource use for pediatric low-grade glioma care: a cohort of linked electronic health records and claims data. ASCO 2023. [PDF]
Chart audit in pediatric low-grade glioma: molecular testing and treatment patterns. ASPHO 2023. [PDF]
pLGG disease burden and healthcare utilization: linked claims and EHR data study. ASPHO 2023. [PDF]
Clinical activity of the type II pan-RAF inhibitor tovorafenib in BRAF-fusion melanoma. EADO 2023. [PDF]
FIREFLY-1 (PNOC 026): A phase 2 study to evaluate the safety and efficacy of tovorafenib (DAY101) in pediatric patients with RAF-altered recurrent or progressive low-grade glioma or advanced solid tumors. ASCO 2022. [PDF]
FIREFLY-1 (PNOC026): Phase 2 study of pan-RAF inhibitor tovorafenib in pediatric and young adult patients with RAF-altered recurrent or progressive low-grade glioma or advanced solid tumors. SNO 2022. [PDF]
LOGGIC/FIREFLY-2: A phase 3, randomized trial of tovorafenib vs. chemotherapy in pediatric patients with newly diagnosed low-grade glioma harboring an activating RAF alteration. SNO 2022. [PDF]
Activity of pan-RAF inhibitor DAY101 in a pediatric patient with a recurrent spindle cell sarcoma harboring a novel SNX8-BRAF gene fusion. CTOS 2021. [PDF]
FIRELIGHT: DAY101-102a, a phase 2 subprotocol of DAY101 monotherapy for patients with recurrent, progressive, or refractory solid tumors with an activating BRAF gene fusion. SMR 2021. [PDF]
Prolonged complete response to the pan-RAF inhibitor DAY101 in a patient with an NRAS-mutated acral lentiginous melanoma. SMR 2021. [PDF]
Scientific Publications
Tovorafenib effective against low-grade gliomas harbouring BRAF fusions. Nat Rev Clin Oncol. 2024 Feb;21(2):83. [Source]
The type II RAF inhibitor tovorafenib in relapsed/refractory pediatric low-grade glioma: the phase 2 FIREFLY-1 trial. Nat Med. 2024 Jan;30(1):207-217. [Source]
LOGGIC/FIREFLY-2: a phase 3, randomized trial of tovorafenib vs. chemotherapy in pediatric and young adult patients with newly diagnosed low-grade glioma harboring an activating RAF alteration. BMC Cancer. 2024 Jan 30;24(1):147. [Source]
Activity of Type II RAF Inhibitor Tovorafenib in a Pediatric Patient With a Recurrent Spindle Cell Sarcoma Harboring a Novel SNX8–BRAF Gene Fusion. JCO Precis Oncol. 2023 Jul:7:e2300065. [Source]
Phase 1 study of the pan-RAF inhibitor tovorafenib in patients with advanced solid tumors followed by dose expansion in patients with metastatic melanoma. Cancer Chemother Pharmacol. 2023 Jul;92(1):15-28. [Source]