Can Famotidine Treat COVID-19?
Preliminary evidence suggests that prescribing famotidine to patients hospitalized with COVID-19 more than halves the risk of death or need for a ventilator. In addition, famotidine also works for the milder form of COVID-19, significantly speeding up recovery.
Famotidine is a popular over-the-counter medication, well known under the brand name Pepcid, universally used for treating heartburn, gastric and duodenal ulcers, erosive gastroduodenitis, reflux esophagitis, and dyspepsia.
Nevertheless, it is too early to have high hopes for famotidine, much less rush to the pharmacy, buying up all its stock. Until the results of randomized controlled trials have been collected, it makes absolutely no sense to place big bets on Pepcid. What to say, if the COVID-19-suffering pandemic world was unequivocally confident in the therapeutic efficacy of the antimalarial hydroxychloroquine, but the results showed its utter uselessness in the fight against the new coronavirus SARS-CoV-2. Again, it has not yet been established exactly at what stage of coronavirus disease and at what dose it is best to use famotidine.
Yes, prophylactic vaccines that protect against coronavirus infection and/or prevent COVID-19 development are available. And these vaccines have demonstrated ridiculously high efficacy, preventing the disease in 95% of cases of infection. However, the need for new medicines for treating COVID-19 has not disappeared.
Famotidine and Coronavirus: Unexpected Discovery
The pharmaceutical industry continues to evaluate a large number of existing drugs in the hope that they can be repurposed to fight the COVID-19. Some, like Gilead Sciences’ Veklury (remdesivir), work directly by blocking the virus’ replication. Others, such as Actemra/RoActemra (tocilizumab) and Olumiant (baricitinib) promoted by Roche and Eli Lilly/Incyte as well as dexamethasone are designed to suppress the overactive immune response leading to the severe complications of COVID-19.
There are also very original approaches. For example, the over-the-counter famotidine, a widely used antagonist of the histamine H2 receptor, has received considerable attention.
The scientific world became interested in famotidine after reports from China: people who took famotidine as part of chronic heartburn therapy successfully survived the COVID-19 challenge. In contrast, those who treated heartburn symptoms with other drugs, including cimetidine or omeprazole, died of complications of coronavirus infection.
Statistically, this was as follows: Chinese patients hospitalized for COVID-19 complications (n=6212) died at a rate of 14% if they followed a course of famotidine, and twice as likely at 27% if they followed therapy with any other antacid drug that suppresses gastric acid secretion.

Clinical Trials’ Landscape of Famotidine for COVID-19 Treatment
Famotidine: The Major Study
In early April 2020, the NCT04370262 phase 3 (randomized, double-blind, multicenter) clinical trial testing the safety and efficacy of adding famotidine to standard therapy in patients (n=942) hospitalized with moderate-to-severe COVID-19 was launched at Northwell Health, the largest hospital system in New York.
Famotidine was administered intravenously 3 times daily at a dose of 120 mg for a maximum of 14 days or until hospital discharge. The cumulative daily dose of intravenous famotidine was 360 mg, equivalent to a giant 720 mg dose of oral famotidine.
Patients with renal insufficiency (creatinine clearance < 50 ml/min) were excluded from the study, because high doses of famotidine, which persists long enough in the body, may lead to cardiovascular complications due to a low risk of QTc interval prolongation.
The primary endpoint of the study was the mortality after 30 days of hospitalization.
Initially, the standard therapy of COVID-19 in this clinical trial involved hydroxychloroquine, but it was later abandoned because of the accumulating evidence of its futility. Instead, remdesivir was used.
As of April 2021, no results have been published on the outcomes of NCT04370262. It is possible that the researchers were unable to recruit the proper number of participants.
Famotidine: It Doesn’t Hurt to Do It Again
In late January 2021, Northwell Health, in collaboration with Cold Spring Harbor Laboratory (CSHL), decided to repeat its attempt to test the validity of famotidine for the treatment of COVID-19.
This time they launched the phase 2 (randomized, double-blind, placebo-controlled) clinical trial NCT04724720, which will probe the therapeutic efficacy of famotidine in patients (n=84) with mild-to-moderate symptoms of COVID-19, confirmed and not requiring hospitalization, in a completely virtual setting (participants are at home and report to the investigators remotely).
Patients who will receive a placebo or oral famotidine at a dose of 240 mg once daily for up to 14 days will be required to perform regular self-examinations and send the results over the Internet. Subjects will be given an Apple iPad with a special app to record data collected by a Bluetooth-enabled scale, thermometer, fitness tracker, spirometer, thermometer, and pulse oximeter. The primary endpoint is set by the cumulative incidence of COVID-19 symptom resolution during 28 days.
As of April 2021, no results have been published on the outcomes of NCT04724720.
Famotidine: Bangladesh Attempt
In August 2020, the NCT04504240 phase 3 (randomized, open-label, multicenter) clinical trial was initiated at Bangladesh’s Chattogram General Hospital to test the addition of oral famotidine (40–60 mg every 8 hours) to standard therapy in COVID-19 patients (n=200) whose disease is either mild to moderate (outpatient care) or moderate to severe (requiring hospitalization).
Two primary endpoints were established, taken within 30 days after randomization: time to clinical improvement and time to symptomatic recovery.
As of April 2021, no results have been published on the outcomes of NCT04504240.
Famotidine: Intriguing Antioxidant
In October 2020, Prisma Health, South Carolina’s largest private non-profit healthcare system, launched the NCT04545008 phase 1 (randomized, open-label) clinical trial among outpatients (n=42) who recently experienced SARS-CoV-2 infection and who will be treated with oral famotidine and N-acetylcysteine (NAC), a mucolytic, expectorant, and antioxidant, in various combined doses. Thus, the combined daily dose of famotidine may be 60, 120, or 240 mg, and NAC may be 1,800, 3,600, or 5,400 mg.
As of April 2021, no results have been published on the outcomes of NCT04545008.
Famotidine: Power in Dietary Supplements
In November 2020, the nonprofit organization ProFact launched the PROFACT-01 (NCT04621149) phase 2 clinical trial (randomized, double-blind or open-label groups) among outpatients (n=120) with a confirmed diagnosis of COVID-19 and its symptoms manifesting within 7 days.
Subjects received oral famotidine along with various over-the-counter complexes of chlorine dioxide, lactoferrin, green tea extract, and zinc acetate for 7 days.
As of April 2021, no results have been published on the outcomes of NCT04621149.
Famotidine: Vitamins Abandoned
The CDFCOV19 (NCT04565392) phase 4 (randomized, open-label) clinical trial was scheduled to begin in December 2020 to examine the feasibility of prescribing famotidine and vitamin drugs in the earliest stages of COVID-19 to prevent worsening of the disease course or avoid the need for hospitalization.
Outpatients (n=216) who experienced symptomatic COVID-19 for no longer than 4 days were to be offered two therapeutic regimens: either 20 mg of famotidine in the morning and evening or 20 mg of famotidine in the morning only; both in either case on a background of 2000 IU of vitamin D3 and 1000 mg of vitamin C (morning) and 1000 mg of vitamin C (evening).
Later in January 2021, however, study sponsor Dr. Pyke’s Supplement reformatted its protocol when the vitamins were abandoned entirely. Pepcid4COV19 will study only famotidine among 150 people. Famotidine (or placebo) is administered 20 mg in the morning and evening on the first day and then, if no improvement in well-being is noted, 20 mg every 8 hours. Famotidine therapy will last for up to 30 days in a row. The study is done entirely remotely.
As of April 2021, no results have been published on the outcomes of NCT04565392.
Famotidine Attacks COVID-19: Preliminary Evidence
Glimpse into the Past
In early May 2020, researchers at Columbia University published a preprint revealing the clinical benefits of famotidine. A retrospective cohort study of patients hospitalized with COVID-19 (n=1620), of whom 5.1% (n=84) received famotidine within 24 hours of admission to the hospital, found that use of the drug provided a 58% reduction in the cumulative risk of clinical deterioration leading to death or need for endotracheal intubation (adjusted hazard ratio [aHR] 0.42 [95% CI: 0.21–0.85]). There was a 70% reduction in the risk of death specifically (aHR 0.30 [95% CI: 0.11–0.80]).
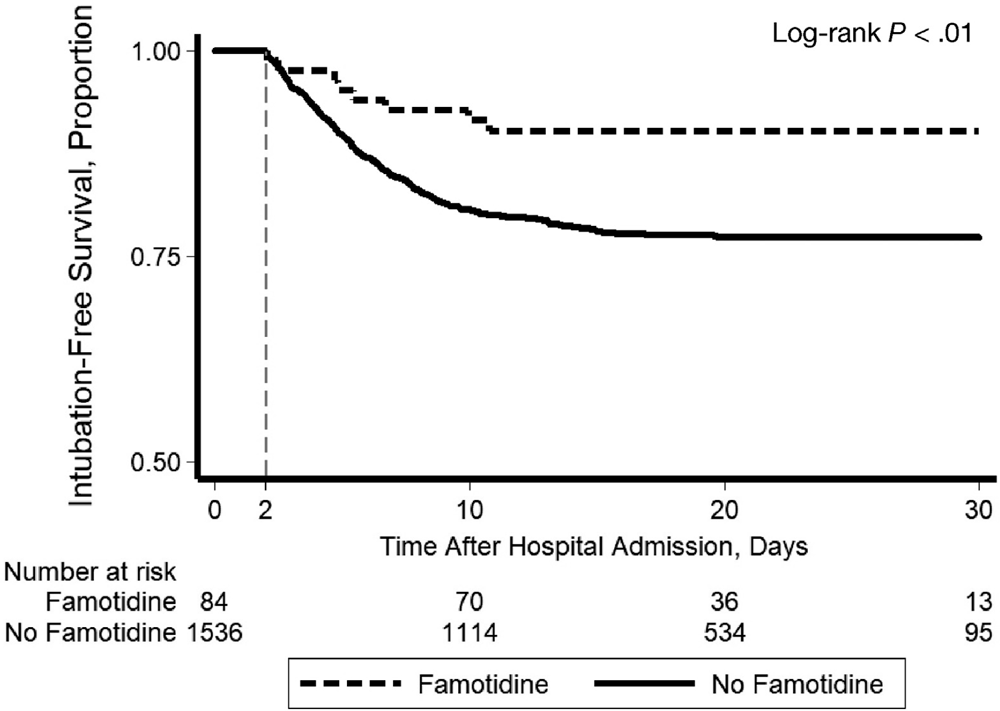
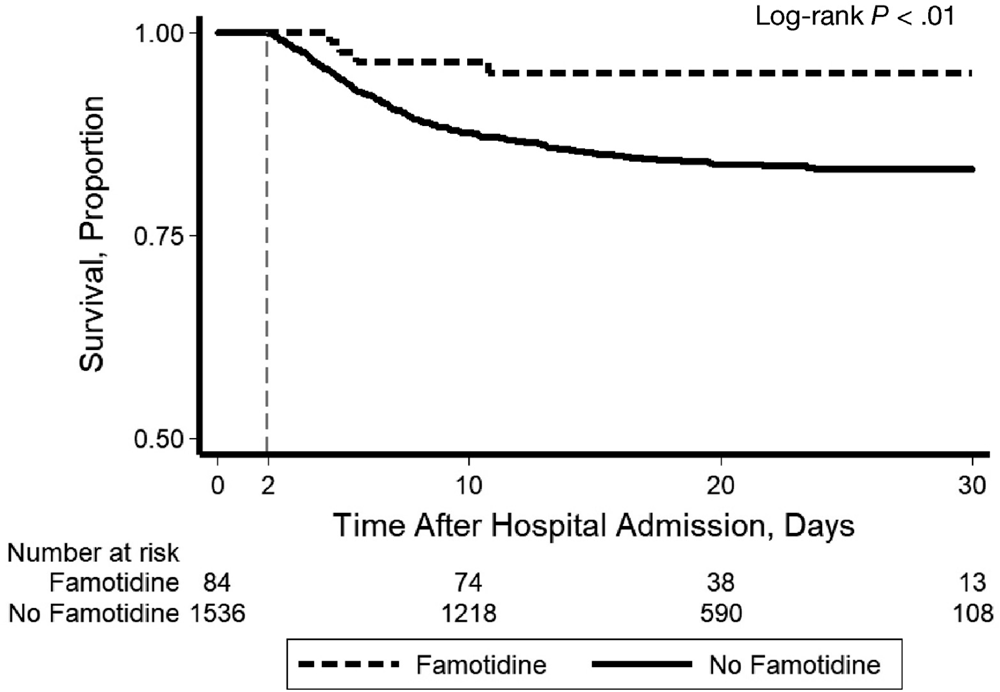
Regarding the route of administration, most patients received famotidine orally (28% of patients received it intravenously). Regarding the route of administration, most patients received it orally (28% of patients received it intravenously). The pattern of daily famotidine dosage was as follows: 47% of patients were prescribed 20 mg, 35% were 40 mg, and 17% were 10 mg. The total median drug dose obtained over a median of 5.8 days was 136 mg (63–233 mg).
After balancing baseline patient characteristics using a propensity score method, the therapeutic benefit of famotidine was maintained: the above cumulative risk reduction came out to 57% (HR 0.43 [95% CI: 0.21–0.88]); considered to be more than twofold. At the same time, the use of proton pump inhibitors had no effect on reducing the likelihood of dying or being put on a ventilator.
The results of the analysis were subsequently reported in a peer-reviewed medical journal. It is believed that the protective effect of famotidine in confronting COVID-19 is seen in the inhibition of cytokine release syndrome.
Partial Excerpts
In early June 2020, an analysis of ten individual cases of famotidine use in patients with COVID-19 occurring in a form that does not require hospitalization was proposed. Significant improvement in disease symptoms (cough, difficulty breathing, fatigue, loss of smell, etc.) within 24–48 hours after initiation of famotidine therapy was demonstrated. The most common famotidine prescribing regimen (n=6) relied on oral administration of 80 mg of the drug three times daily for a median of 11 days (5–21 days).
Notably, the apparent improvement in clinical status after 48 hours after initiation of famotidine therapy was independent of the length of the preceding symptomatic period of infection. In other words, it did not matter at what stage of the disease the therapy was started. Although, it is possible that the improvement in symptoms in the later stage of the disease was simply due to the natural course of COVID-19.
The July 2020 preprint noted 25 consecutive cases of 100% survival in patients hospitalized with coronavirus disease (80% of patients were obese and half had a severe course of COVID-19) that demonstrated both improved radiological outcomes and statistically significant improvement in several clinical, biomarker, and renal function measures. These were patients who received oral famotidine and celecoxib, a selective cyclooxygenase-2 (COX-2) inhibitor, in addition to standard therapy for COVID-19 (no later than 24 hours after admission). The former was administered four times a day at 80 mg; the latter was first at a loading dose of 400 mg and then at 200 mg twice a day.
Compilation of Everything
In late September 2020, a preprint appeared that was the first most comprehensive systematic review and meta-analysis of the role of famotidine in the treatment of covid. It is stated that the existing evidence base demonstrates a potentially favorable therapeutic effect of famotidine in the task of reducing mortality in moderate to severe coronavirus infection. Nevertheless, robust clinical validation is still needed to definitively confirm it.
And More
A systematic review of the literature on famotidine in the COVID-19 setting was published in early November 2020. It concluded that the positive therapeutic effects of famotidine are not due to a direct effect on the new coronavirus SARS-CoV-2, but to an H2 receptor-mediated immunomodulatory effect on mast cells secreting histamine and cytokines.
Largest Analysis
In early April 2021, a preprint appeared that attempted to address the controversy surrounding famotidine in the treatment of COVID-19 because some studies suggest that it works, while others, on the other hand, argue that it is of no benefit. To do this, the authors analyzed data from as many as 22,560 patients treated with H1/H2 receptor antagonists with a special focus on 1,379 severe cases requiring respiratory support.
In patients on respiratory support, the use of famotidine was found to statistically significantly reduce the risk of death: risk difference (RD) −6.7% (95% CI: −12.2 — − 1.3; p=0.0152), risk ratio (RR) 0.80 (95% CI: 0.68–0.96), odds ratio (OR) 0.73 (95% CI: 0.57–0.94).
Curiously and unexpectedly, adding aspirin to famotidine leads to even better outcomes: RD −13.1% (95% CI: −20.5 — −5.7; p=0.0006), RR 0.67 (95% CI: 0.54–0.85), OR 0.55 (95% CI: 0.39–0.78). In other words, the combined use of famotidine and aspirin reduced the risk of death from COVID-19 complications by an impressive one-third.
Famotidine Against SARS-CoV-2: Mechanism of Action
Medical science is trying to clarify exactly how famotidine works in the setting of infection with the new coronavirus SARS-CoV-2. And there are still too many possible explanations to choose the unequivocally correct one.
Computer modeling
Chinese investigators turned to computational methods to explore SARS-CoV-2 genes to predict the structures of viral proteins and performed a computational screening of existing drugs to determine which ones could potentially act on these protein targets. Famotidine was found to inhibit 3-chymotrypsin-like protease (3CLpro), also known as SARS coronavirus main protease (Mpro) or C30 endopeptidase, an important enzyme involved in the synthesis of nonstructural viral proteins necessary for its replication. Blocking this protease leads to the formation of an immature and unable-to-replicate virus.
Experts from the Canadian Molecular Forecaster, which develops scientific software, and specialists from the classified project DOMANE (Discovery of Medical Countermeasures Against Novel Entities) at the U.S. Department of Defense (DoD), engaged in the repurposing of existing drugs, have virtually tested a library of 2.7 thousand approved drugs and nutraceuticals to identify which ones fit into a computer model of the virus’ papain-like protease (PLpro), another key protein involved in the SARS-CoV-2 replication cycle. Famotidine appeared to interact with this enzyme, binding and blocking it.
But the National Center for Advancing Translational Sciences (NCATS) team at the US National Institutes of Health (NIH) did not find that famotidine had any clear antiviral activity in SARS-CoV-2 infection. Although it is argued, this does not at all mean that it does not make sense to clinically test famotidine in the context of COVID-19.
It was later found that, first, famotidine does not bind to SARS-CoV-2 proteases, second, it has no direct inhibitory effect on the new coronavirus, and third, it does not affect sigma-1 (σ1R) and sigma-2 (σ2R) receptors, whose regulation is characterized by antiviral effects. Nevertheless, a hypothesis has been proposed according to which the use of famotidine is still justified in COVID-19.
Cytokine Storm Hypothesis
Activation and degranulation of mast cells in response to infection with the SARS-CoV-2 may be thought to explain some of the major pathological cascades and much of the unusual symptoms of COVID-19. Many of the unique and disease-specific symptoms (anosmia, dyspnea, cough, fever, hypoxia) observed early in the infection are consistent with the known effects of histamine release. The proposed model is deeply consistent with the clinical signs and symptoms in mast cell activation syndrome (MCAS). Similarities with dengue hemorrhagic fever and associated shock syndrome are noted in the late stage of COVID-19. Cardiac events and strokes are very similar to those of Kounis syndrome.
The simple and obvious explanation for the therapeutic activity of famotidine in COVID-19 lies in its mechanism of action. The drug works through antagonism and inverse agonism of histamine signaling by binding to the histamine H2 receptor. It prevents the degranulation of mast cells, which would release hundreds of signaling molecules (including histamine, bradykinin, heparin, tryptase, cytokines) in response to inflammatory and allergic reactions, affecting cellular and basal membrane function, glycocalyx, and the integrity of tight intercellular contacts. The emerging cytokine release syndrome, or cytokine storm, determines the course of COVID-19 in a severe and even life-threatening form. Famotidine prevents and mitigates this condition.
COVID-19 symptoms affect several organ systems, but respiratory failure caused by acute respiratory distress syndrome (ARDS) is the most common cause of death. RNA expression profiles of cells involved in lung anatomy and function indicate multiple ACE2/TMPRSS2-positive epithelial and endothelial cell types susceptible to the new SARS-CoV-2 coronavirus. Because these cells and others, being histamine H1 and H2 receptor-positive, respond to local histamine release following mast cell degranulation, there is clinical validity in prescribing famotidine. Among the cells most likely to respond to famotidine are type II pneumocytes, smooth muscle cells, pericytes, myeloid granulocytes (mast cells, neutrophils, eosinophils).
Hydrochloric Acid Hypothesis
According to the September 2020 preprint, increased acidity of gastric juice leads to increased expression of the angiotensin-converting enzyme 2 (ACE2) receptor on host cells. Since it is the ACE2 receptor that is being exploited by the new SARS-CoV-2 coronavirus as a primary entry point into infected cells, the rise in ACE2 expression provides the virus with a greater opportunity for infection.
This finding was revealed by analyzing tissue samples from patients with Barrett’s esophagus or gastroesophageal reflux disease (GERD). Individuals with these diseases were found to be prone to a more severe course of COVID-19 because their tissue ACE2 expression is presumably elevated due to lower intracellular pH values.
Nevertheless, it remains unclear why prescribing proton pump inhibitors that reduce gastric acidity (which should result in inhibition of ACE2 expression) worsens (the risk of death increases two to threefold) the clinical outcomes of COVID-19 patients. In contrast, the use of antacid famotidine improves them.
Bradykinin Storm Hypothesis
In the summer of 2020, the Summit supercomputer, an IBM-built system at the Oak Ridge National Laboratory (ORNL) in Tennessee and the second-fastest computer in the world, had revealed a new theory about how COVID-19 impacts the body.
Once the new coronavirus SARS-CoV-2 has infected the organism, it begins to promote an abnormally high increase in ACE2 receptor expression in places where it would normally be at a low or moderate level. This leads to a significant rise in bradykinin levels, which, according to this theory, is the main contributor to all the major manifestations of COVID-19.
Thus, bradykinin accumulation is reflected by increased vascular permeability: the lungs fill up with fluid, and the immune cells penetrating them trigger the process of large-scale inflammation of lung tissue. Bradykinin promotes the synthesis of hyaluronic acid, which, by forming a hydrogel in the lumen of the alveoli, causes respiratory problems and makes ventilation ineffective. Because bradykinin is closely linked to the renin–aldosterone system (RAS), which controls heart contractions and blood pressure, bradykinin storms are mirrored by arrhythmia, decreased blood pressure, weakness, and fatigue. Increased bradykinin levels explain the neurological effects in patients with COVID-19: dizziness, seizures, delirium, and stroke, all of which can develop equally due to leaking blood vessels in the brain as to the breakdown of the blood-brain barrier.
It is possible that the curative effect of famotidine is related to the inhibition of bradykinin-containing mast cell degranulation.
Famotidine and Cimetidine: Why the Former and Not the Latter?
If famotidine is effective for COVID-19, why are other popular H2 blockers like cimetidine useless?
First, famotidine, a selective blocker of the histamine H2 receptor, has an affinity of 14 nM, which is much lower than the 590 nM of cimetidine. At the same time, famotidine has strong inverse agonist activity with respect to the histamine H2 receptor (reduces basal activity by 75%) with a potency of 33 nM; the positive effect of famotidine is seen in the form of desensitization and internalization of the receptor, as well as promotion of ERK1/2 phosphorylation. In other words, administration of cimetidine (at least orally) leads to a decidedly insufficient systemic concentration of the drug to effectively bind the histamine H2 receptor.
Second, famotidine, unlike cimetidine, blocks heterodimeric G protein Gs signaling, that is, it actually acts as a partial agonist of beta-arrestin recruitment with an efficiency of approximately 15% of that for histamine and a half-maximal effective concentration (EC50) of 105 nM. Famotidine promotes useful circuits of physiological events in COVID-19.
Third, famotidine activates the chemokine receptors CCR2L and CXCR3, thereby stimulating beneficial immune cell mobilization. This explains why famotidine does not exhibit direct antiviral action in vitro: because immunocytes were not present in experiments on Vero E6 cell lines.
Famotidine for Treatment of COVID-19: With Increasing Eager Anticipation
If the pathophysiological pattern of COVID-19 is indeed due in part to dysfunctional mast cell degranulation, then existing marketed drugs used in the therapy of mast cell-related diseases will help to restrain this process. Such potentially suitable drugs include mast cell activity stabilizers, other histamine antagonists (e.g., its H1 and H4 receptor blockers), leukotriene and its receptor antagonists, anti-inflammatories (e.g., those against inflammatory bowel disease), and mast cell activation inhibitors.
If the above is clinically proven, a workable COVID-19 treatment and prophylaxis regimen emerges, including direct SARS-CoV-2 antivirals like remdesivir.
A plateau of famotidine concentrations sufficient for successful H2 receptor antagonism (and reverse agonism) is easily achieved by taking very inexpensive oral tablets at a safe dose. In the NCT04370262 clinical trial, famotidine was administered intravenously at a dose that was more than 20 times the half-maximal inhibition concentration (IC50) required for histamine H2 receptor antagonism. However, this is clearly excessive.
Taking a dose of 40–60 mg every 8 hours is sufficient to maintain adequate levels of famotidine in the body. Since famotidine is mainly excreted by the kidneys, higher doses require their adequate functional status.
Famotidine: Donald Trump Is Not Afraid of COVID-19
Donald Trump, who fell ill with COVID-19 in early October 2020, has been treated with an impressive array of drugs. In addition to Veklury, dexamethasone, and a couple of experimental monoclonal antibodies from Regeneron Pharmaceuticals, the former U.S. president was treated with zinc, vitamin D, melatonin, aspirin, and famotidine.
Famotidine Against Coronavirus: Hurry Up!
The good news came from Russia. Physicians at the Kirishi District Hospital (Leningrad Oblast) were convinced that the use of famotidine during treatment of patients hospitalized with moderate to severe COVID-19 halted the worsening of the severity of the coronavirus infection. Encouragement of the outcome led to the publication of an open letter to fellow physicians.
Famotidine: Cheap but Not Available
Without regard to the lack of reliable evidence of famotidine’s anti-COVID-19 activity, there is a clear shortage. Thus, in early May 2020, the United States faced a shortage of famotidine once it became known that it could sort of help in the fight against coronavirus. The acute shortage of this penny-pinching drug continues to this day.
Famotidine for Coronavirus: First Doubts
A preprint from October 2020 spoke strongly against prescribing famotidine to COVID-19 patients. A retrospective study found that the addition of famotidine (started within 24 hours of admission) to standard therapy for patients hospitalized with COVID-19 demonstrated neither additional risk nor additional benefit to the 30-day mortality rate. However, among those who did not take famotidine at home but received it in the hospital, the risk of mortality increased by 77%.
This was true without regard to adverse reactions and possible confounding factors in the COVID-19 settings, such as older age, obesity, smoker status, risky comorbidity, severe COVID-19, use of the toxic hydroxychloroquine, etc.
The analysis included data from 1,156 patients, of whom 35.5% (n=410) received famotidine.
The authors of the study, however, emphasize a number of shortcomings and flaws in their work, which do not allow a generalized conclusion about famotidine. First, the observational design fails to identify causality and may be biased. Second, there was no analysis of serum biomarkers or viral load to assess the anti-inflammatory and antiviral properties of famotidine. Finally, over 95% of the cohort patients received low- or medium-dose famotidine, meaning there is no way to determine whether famotidine at high doses is useful.
Famotidine for Coronavirus: Second Skepticism
A preprint published in late March 2021 presenting a systematic review and meta-analysis of clinical outcomes during famotidine therapy of hospitalized patients with COVID-19 made it clear that prescribing this drug was not associated with a reduced risk of death, need for intubation, and/or intensive care interventions. Although a certain favorable trend was still observed. The authors, however, emphasize considerable heterogeneity across studies and therefore conclude that further clinical trials of famotidine are needed.
Famotidine and COVID-19: For Further Reading
Efficacy of famotidine for COVID-19: a systematic review and meta-analysis. [source]
The effect of famotidine on hospitalized patients with COVID-19: a systematic review and meta-analysis. [source]
Famotidine use is associated with improved clinical outcomes in hospitalized COVID-19 patients: a propensity score matched retrospective cohort study. Gastroenterology. 2020 Sep;159(3):1129-1131.e3. [source]
Famotidine use and quantitative symptom tracking for COVID-19 in non-hospitalised patients: a case series. Gut. 2020 Sep;69(9):1592-1597. [source]
Hospitalized COVID-19 patients treated with celecoxib and high dose famotidine adjuvant therapy show significant clinical responses. [source]
Famotidine use is not associated with 30-day mortality: a coarsened exact match study in 7158 hospitalized COVID-19 patients from a large healthcare system. Gastroenterology. 2021 Feb;160(3):919-921.e3. [source]
Histamine receptors and COVID‑19. Inflamm Res. 2021 Jan;70(1):67-75. [source]
COVID-19: famotidine, histamine, mast cells, and mechanisms. Res Sq. 2020 Jun 22;rs.3.rs-30934. [source]
A mechanistic model and therapeutic interventions for COVID-19 involving a RAS-mediated bradykinin storm. Elife. 2020 Jul 7;9:e59177. [source]
List of Famotidine’s Brand Names
Famotidine, being more than a popular drug, is available for sale in all countries of the world. It is produced by everyone who is not lazy. For reference purposes, we have prepared a list of brand names of famotidine. And it turned out to be huge (almost 300 trademarks)!