Highlights
Taking the antibiotic doxycycline within 72 hours of unprotected (condomless) sexual intercourse reduces the risk of contracting bacterial sexually transmitted infections (STIs) such as gonorrhea, chlamydia and syphilis by more than 60%.
The proposed method of STIs prevention is experimental. If it receives regulatory approval, it will likely be mainly among people at high risk for STIs.
Post-exposure prophylaxis (PEP) with publicly available and inexpensive doxycycline offers new prospects for preventing STIs, which in some cases may occur without particularly distressing and discouraging symptoms, resulting in the disease being left untreated. This poses risks of both further progression of the infection and its transmission from the sick to the healthy.
Details
The DoxyPEP (NCT03980223) phase 4 ( randomized, open-label, multicenter) clinical trial examined the hypothesis that doxycycline administration after unprotected sexual intercourse is warranted for the prevention of sexually transmitted infections (STIs), including gonorrhea, chlamydia, and syphilis.
Adult men who have sex with men (MSM) and transgender women invited to participate in the trial had to be, first, either HIV-positive (cohort 1) or HIV-negative and adhering to pre-exposure HIV prophylaxis (cohort 2) and, second, have a past history of gonorrhea, chlamydia, or early syphilis. These selection criteria were established because of the high risk of STIs in this population.
Among the main characteristics of the subjects (n=501): median age 38 years (32–47); median number of sexual partners in the past 3 months was 9 (4–17); STIs in the past 12 months were gonorrhea in 69% of participants, chlamydia in 58%, and syphilis in 20%; psychoactive substance use in the past 3 months was addressed by 59% of subjects, of which stimulants (methamphetamine, cocaine, crack) were used by 59%, amyl nitrite (poppers) by 45%, and other substances (ecstasy, gamma-hydroxybutyric acid, ketamine) by 32%.
In the one-year follow-up, participants after unprotected sexual intercourse (oral or anal) were asked either to do nothing or to take doxycycline once at a dose of 200 mg, preferably in the first 24 hours or at most within 72 hours, no more than once every 24 hours regardless of the number of sexual acts occurring during this period.
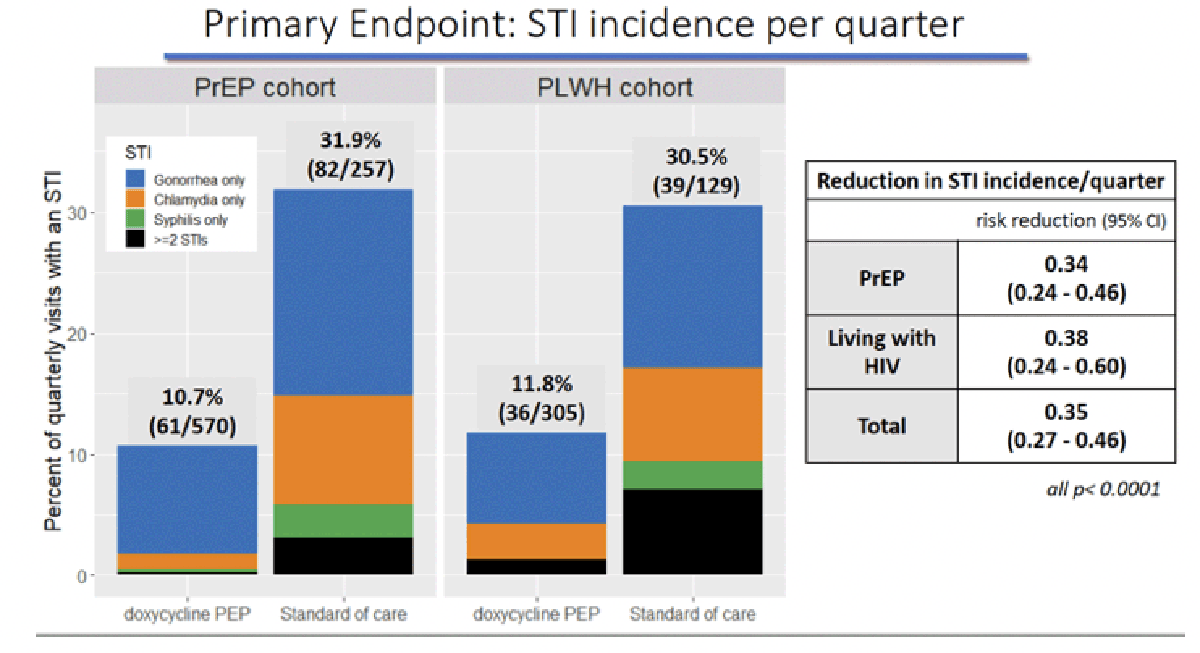
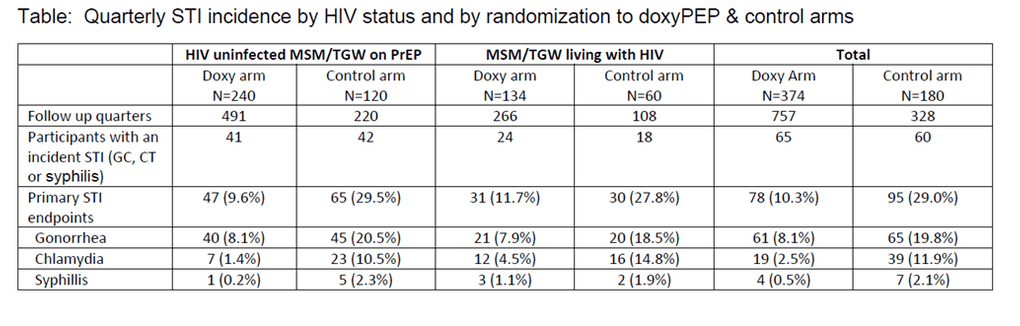
Post-exposure administration of doxycycline was found to provide a 65% reduction in risk of STIs per quarter relative to no preventive measures: risk reduction (RR) 0.35 (95% CI: 0.27 to 0.46; p<0.0001). The protective efficacy of doxycycline in cohorts 1 and 2 was 66% and 62%: RR 0.34 (95% CI: 0.24 to 0.46) and RR 0.38 (95% CI: 0.24 to 0.60).
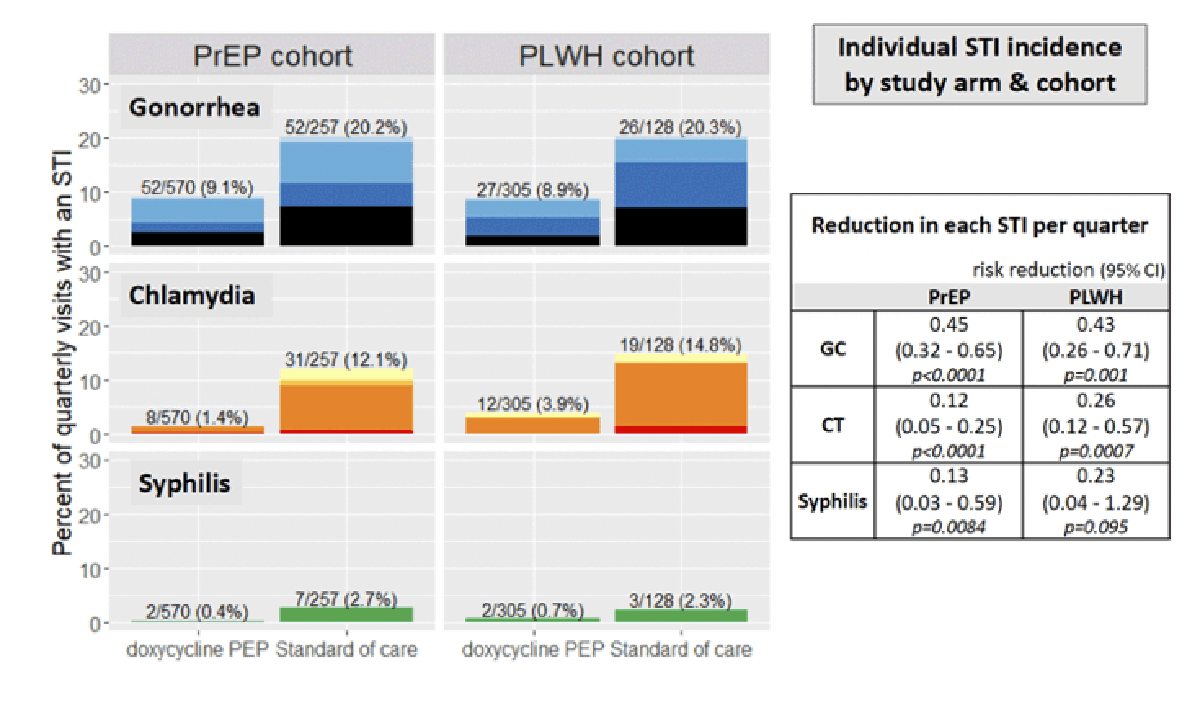
In terms of preventing a specific STI, the quarterly risk of acquiring gonorrhea, chlamydia, or syphilis was reduced by 55% and 57%, 88% and 74%, and 87% and 77% in cohort 1 and cohort 2, respectively.
Expert Comments
The idea of doxycycline as protection against STIs was tested in a small pilot study DPMSM (NCT02257658) among high-risk HIV-infected MSM. Doxycycline 100 mg daily as pre-exposure prophylaxis (PrEP) for gonorrhea, chlamydia, and syphilis was demonstrated to be effective. However, such preventive continuous administration of doxycycline is unlikely to be justified from all perspectives. [1]
A companion study to the IPERGAY (NCT01473472) phase 3 clinical trial among MSM was then conducted. It found that doxycycline at a dose of 200 mg taken within 24 hours of unprotected sexual intercourse (PEP) reduced the risk of STIs by 47% (p=0.008), including the risk of chlamydia by 70% (p=0.006), syphilis by 73% (p=0.047), and gonorrhea by 17% (p=0.52). [2]
Experts’ opinions regarding the use of doxycycline as a prophylactic drug are divided. Along with rave reviews stemming from the efficacy and safety of this drug, there is an opinion that such use of doxycycline will increase the development of antibiotic resistance in gonococcus (Neisseria gonorrhoeae). However, even if N. gonorrhoeae resistance to antibiotics increases, this essentially means little. First, doxycycline will only be used in high-risk groups, which are small relative to the entire population. Second, current approaches to treating gonorrhea involve the use of other classes of antibiotics. Third, N. gonorrhoeae is often already resistant to doxycycline, as was evidenced in the IPERGAY conducted in France, where tetracycline resistance to gonococcus is decently high. [3]
As for Chlamydia trachomatis and Treponema pallidum, they have not yet evolved enough to make chlamydia infection and syphilis resist doxycycline due to the possible (but not obligatory) development of resistance to tetracyclines.
There remains a certain risk of developing drug resistance in side bacteria, although in the context of doxycycline this is not particularly relevant. For example, the treatment of inflammatory diseases of the urogenital tract caused by Mycoplasma genitalium is unlikely to be treated with doxycycline due to its lack of effectiveness. Many other antibiotics are available for eradication of methicillin-resistant Staphylococcus aureus (MRSA). The issue with commensal and mutualistic bacteria, including those belonging to the microbiome, remains open.
Strictly speaking, doxycycline prophylaxis definitely needs further in-depth study of the risks of developing antibiotic resistance.
Be that as it may, the benefits of doxycycline for post-exposure prophylaxis of STIs currently outweigh the risks, among a high-risk population.
Meanwhile, the viability of doxycycline prophylaxis for gonorrhea, chlamydia, and syphilis is being studied in several other clinical trials: the Australian Syphilaxis (NCT03709459), Canadian DISCO (NCT04762134), French DOXYVAC (NCT04597424), American PEACH (NCT05072093), and Kenyan dPEP-KE (NCT04050540). All studies are conducted among MSM, except for the last one, which is performed among women.